The Integration of Character Structure and Personality Organization
Ann Coleman
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2024 (34), 55–81
https://doi.org/10.30820/0743-4804-2024-34-55 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comFor most of us the experience of being a person is so familiar, so unified, and so continuous that it’s difficult not to take it for granted. But we shouldn’t take it for granted …the basic background experience of being a unified self is a rather fragile construction …
Dr. Anil Seth
Abstracts
Theories of both Personality Organization (PO) and Bioenergetic Character Analysis (BA) are born from Psychoanalysis. Due to the influence of a medical model of understanding and treating mental health disorders PO and BA have been taught and developed separately. This article explains PO to the Bioenergetic audience, via the Psychodynamic Diagnostic Manual, Second Edition (PDM-2), and proposes a circumplex model for how to integrate the two theories. A psychoanalytic understanding of how people can organize their sense of self in a borderline or psychotic way is described, in contrast to a medical model of viewing borderline and psychotic experiences as discreet disorders. A concept of the self is defined and provides the basis for the integration of theories. Dynamics and traits for borderline and psychotic organization are described and contrasted so that a clinician can identify the difference between the two. A case study is presented to demonstrate how the integration of the two theories looks in practice.
Keywords: personality organization, character structure, psychoanalysis, PDM-2, circumplex model, sense of self
Integração da Estrutura de Caráter e da Organização de Personalidade (Portuguese)
Tanto a Teoria da Organização de Personalidade (PO) quanto a da Análise de Caráter Bioenergética (BA) têm sua origem na Psicanálise. Por causa da influência do modelo médico de compreensão e tratamento de desordens da saúde mental, PO e BA têm sido ensinadas e desenvolvidas separadamente. Este artigo explica a PO para a comunidade da Bioenergética, através do Manual do Diagnóstico Psicodinâmico – Segunda Edição (PDM 2) e propõe um modelo circumplexo de como integrar as duas teorias. Traz, também, uma compreensão psicanalítica de como as pessoas podem organizar seu senso de self num modo de ser borderline ou psicótico, em contraste com a visão do modelo médico para experiências borderline e psicóticas como desordens discretas. O artigo define um conceito de self como base para a integração das teorias e descreve dinâmicas e traços para as organizações borderline e psicótica, de modo que se possa identificar a diferença entre as duas. Apresenta-se um estudo de caso, para demonstrar como a integração das duas teorias se apresenta na prática.
La integración de la estructura del carácter y de la organización de la personalidad (Spanish)
Las teorías tanto de la Organización de la Personalidad (OP) como del Análisis Bioenergético del Carácter (AB) tienen su origen en el Psicoanálisis. Las teorías OP y AB se han desarrollado y estudiado de forma separada, debido a la influencia del modelo médico de comprensión y tratamiento de los trastornos mentales. Este artículo explica la teoría OP para la comunidad bioenergética, a través del Manual Diagnostico Psicodinámico PDM-2, y plantea un modelo circumplejo sobre cómo integrar las dos teorías. Se expone una comprensión psicoanalítica de cómo las personas pueden organizar su sentido del yo de forma límite o psicótica, en comparación con un modelo médico que considera las experiencias límite y psicóticas como trastornos discretos. Se define el concepto del yo, que proporciona la base para la integración de las teorías. Se detallan y contrastan las dinámicas y los rasgos de la organización borderline y psicótica para que el terapeuta pueda identificar la diferencia entre ambas. Se incluye un estudio de caso para demostrar cómo se ve en la práctica la integración de las dos teorías.
L’integrazione della struttura caratteriale e dell’organizzazione della personalità (Italian)
Dalla Psicoanalisi nascono sia la teoria dell’Organizzazione della Personalità (PO) che l’Analisi Bioenergetica del Carattere (BA). A causa dell’influenza di un modello medico di comprensione e trattamento dei disturbi della salute mentale, PO e BA sono stati insegnati e sviluppati separatamente. Questo articolo spiega la PO al pubblico bioenergetico, tramite il Manuale Diagnostico Psicodinamico, Seconda Edizione (PDM-2), e propone un modello circomplesso su come integrare le due teorie. Viene descritta la comprensione psicoanalitica di come le persone possono organizzare il proprio senso di sé in modo borderline o psicotico, in contrasto con il modello medico che vede le esperienze borderline e psicotiche come disturbi discreti. Viene definito un concetto del sé che fornisce la base per l’integrazione delle teorie. Le dinamiche e i tratti dell’organizzazione borderline e psicotica vengono descritti e messi a confronto in modo che il clinico possa identificare la differenza tra i due. Viene presentato un caso clinico per dimostrare come appare nella pratica l’integrazione delle due teorie.
L’intégration de la structure du caractère et de l’organisation de la personnalité (French)
Les théories de l’organisation de la personnalité (OP) et de l’analyse bioénergétique du caractère (AB) sont issues de la psychanalyse. En raison de l’influence d’un modèle médical de compréhension et de traitement des troubles mentaux, l’OP et l’AC ont été enseignées et développées séparément. Cet article explique la théorie de l’OP au public bioénergétique, par le biais du Manuel de diagnostic psychodynamique, deuxième édition (PDM-2), et propose un modèle circomplexe pour intégrer les deux théories. Une compréhension psychanalytique de la façon dont les gens peuvent organiser leur sens du soi d'une manière borderline ou psychotique est décrite, contrairement au modèle médical qui considère les expériences borderline et psychotiques comme des troubles séparés. Un concept de soi est défini et sert de base à l’intégration des théories. La dynamique et les traits de l’organisation borderline et psychotique sont décrits et comparés afin qu’un clinicien puisse identifier la différence entre les deux. Une étude de cas est présentée pour démontrer comment l’intégration des deux théories se présente dans la pratique.
Die Integration von Charakterstruktur und Persönlichkeitsorganisation (German)
Die Theorien der Persönlichkeitsorganisation (PO) und der Bioenergetischen Charakteranalyse (BA) sind aus der Psychoanalyse hervorgegangen. Aufgrund des Einflusses eines medizinischen Modells zum Verständnis und zur Behandlung psychischer Störungen wurden PO und BA getrennt voneinander gelehrt und entwickelt. In diesem Artikel wird die PO dem bioenergetischen Publikum anhand des Psychodynamischen Diagnosehandbuchs, Zweite Ausgabe (PDM-2), erklärt und ein Circumplex-Modell für die Integration der beiden Theorien vorgeschlagen. Es wird ein psychoanalytisches Verständnis davon beschrieben, wie Menschen ihr Selbstgefühl in einer Borderline-artigen oder psychotischen Weise organisieren können, im Gegensatz zu einem medizinischen Modell, das Borderline- und psychotische Erfahrungen als diskrete Störungen betrachtet. Es wird ein Konzept des Selbst definiert, das die Grundlage für die Integration von Theorien bildet. Dynamiken und Merkmale der Borderline- und psychotischen Organisation werden beschrieben und einander gegenübergestellt, so dass ein*e Kliniker*in den Unterschied zwischen den beiden erkennen kann. Anhand einer Fallstudie wird gezeigt, wie die Integration der beiden Theorien in der Praxis aussieht.
Интеграция структуры характера и организации личности (Russian)
Теории организации личности (ОЛ) и биоэнергетического анализа характера (БА) возникли из психоанализа. Из-за влияния медицинской модели понимания и лечения психических расстройств ОЛ и БА преподавались и развивались раздельно. Эта статья объясняет ОЛ биоэнергетической аудитории с помощью Руководства по психодинамической диагностике (PDM-2), второе издание, и предлагает комплексную модель, как можно объединить две эти теории. Предложено психоаналитическое понимание, как люди могут организовывать свое ощущение себя пограничным или психотическим образом, в отличие от медицинской модели, рассматривающей пограничный и психотический опыт как скрытые расстройства. Дано определение концепции “я”, что обеспечивает основу для интеграции теорий. Динамика и черты пограничной и психотической организаций описаны и сопоставлены таким образом, чтобы клиницист мог определить разницу между ними. Предложено тематическое исследование, демонстрирующее, как интеграция двух теорий выглядит на практике.
性格结构和组织的整合 (Chinese)
人格组织(PO)和躯体动力性格分析(BA)都诞生于精神分析。由于受到理解和治疗心理健康疾病的医学模式的影响,PO 和 BA 一直是分开教授和发展的。本文通过《精神动力学诊断手册第二版》(PDM-2)向躯体动力分析受众解释了PO,并就如何整合这两种理论提出了一个环形模型。描述了精神分析对人们如何以边缘型或精神病的方式组织自体意识的理解,对比了与将边缘型和精神病体验视为独立疾病的医学模式。文中定义了自体的概念,为理论的整合提供了基础,还对边缘型组织和精神病组织的动力和特征进行了描述和对比,以便临床医生能够识别两者之间的区别。并通过对一个案例的研究,展示了两种理论在实践中的整合效果。
Introduction
A few years into opening my private practice I began receiving phone calls from people who explained that they had Bioenergetic Therapy in the past and wanted to step into therapy again. I was lucky enough to be working out of the turn-of-the-century equestrian breeding barn that had been converted into office space in 1971 and was the home of the Michigan Society for Bioenergetic Analysis. Many of my mentors had retired or passed, so it seemed natural that they had found me. It was surprising and humbling at first, but by the 4th call I saw a pattern of people whose defensive capacities were primitive and/or decompensating. They shared with me histories of seriously abusive families of origin, current unstable and enmeshed relationships, and two had the magical thinking that I had a miracle energy cure. Great dismay and inner conflict set in as I believed (and still do) wholeheartedly in the cathartic and transformational power of Bioenergetic Analysis. I had many questions and I set off to find answers to understand what was happening. Six people in total reached out to me with this same presentation. I took client histories, used my knowledge from working in psychiatric hospitals, and discerned that they had severe personality and/or psychotic disorders. I awakened to the fact that my only experience in working with people with personality and psychotic disorders was in a “revolving door” medical-model system that treated them as symptom clusters and pharmaceutical trials rather than people. In all my psychiatric education and experience I had not been taught to provide a long-term treatment to improve quality of life for the people with severe histories.
With my affinity for psychoanalytic theory, I began a journey to understand the etiology of personality disorder and psychosis and find a way of working with people whose self-structure and defenses decompensate. I started with Freud’s original paper On Narcissism: An Introduction (1991), and expanded through psychoanalysis, ego psychology, object relations theory, attachment theory and research, polyvagal theory and research, and neuroscience. I read about the multidimensional and inferential diagnostic assessment of personality that was developed in the broader field of psychoanalysis but had been forsaken and kept out of mainstream psychological treatment in favor of the medical model that had expanded exponentially in the 1950’s until this day. I discovered a psychoanalytic conceptualization and treatment template in the thick book called the Psychodynamic Diagnostic Manual, originally published in 2006, with a second addition, PDM-2, published in 2017. This manual includes what is coined Personality Organization.
Personality Organization views a person through a lens of cognitive and affective processes, identity and relationship, stress resilience and maturity of defenses, self-awareness, and self-direction. The manual has a method for clinicians to assess how well a person functions in these areas. It is a diagnostic framework that has us look at personality in terms of self-structure capacities on a “mental functioning” spectrum from healthy to disordered. I will explain these 4 levels of organization in the main part of this paper. This framework has been developed at the same time but separately from Character Analysis over the decades, and today, it has the potential to both be integrated with and inform our understanding of Character Structure.
As a matter of fact, the second half of the PDM-2 describes and has one assessment of “personality patterns” or what we, as Bioenergetic Analysts, known as “character styles”. This framework has become a guide for me to assess and discern how to work with people who have severe disorders. In this paper I examine how Personality Organization and Character Structure inform one another and can be used together to complete an approach to long term treatment. Let’s start with understanding the fork in the road between the medical model of mental health treatment and psychoanalysis, and where Personality Organization and Bioenergetic Analysis sit in the landscape of treatment.
Some Psychoanalytic History
Bioenergetic Analysis (BA) has clear, direct roots in psychoanalysis by way of Wilhelm Reich who graduated from the University of Vienna and worked in the same collegial group as Sigmund Freud. Reich’s contributions to psychoanalysis of: (a) observing the body as the keeper and manifestation of psychological issues; and (b) the distinction between “symptom neuroses” and “character neuroses”, which is based in and built upon Freud’s drive theory, were just that – contributions to a lush and evolving scientific field (Reich, 1933). As Character Analysis became an area of thought for developing psychoanalysis, there were also many other lines of thought within psychoanalysis, all influencing each other: Ego Psychology, Interpersonal Psychoanalysis, Kleinian Theory, Object Relations Theory, Psychologies of Identity and Self, the Contemporary Freudian Revisionism of Otto Kernberg, and so on (Mitchell & Black, 1995). These theories advanced drive theory to include a person’s subjective experience of themselves, as well as the relational and developmental experiences as they are experienced in the individual psyche. Psychoanalysts discerned the difference between drives and struggles when a developmental phase was interrupted or incomplete and they mapped differential diagnosis of pathologies.
As psychoanalysis evolved in the first half of the 20th century, theory and treatment of mental and personality disorders became influenced by, and intertwined with, scientific research into human behavior. The scientific culture of the time sought quantitative categorization, and this was endemic in the general field of medicine. This dynamic then produced the original Diagnostic and Statistical Manual of Mental Disorders (DSM) in 1952 to “create a single nomenclature for psychopathology” (History of DSM). This compilation and framework of classifying mental health disorders
“embraced a shift from a psychoanalytically influenced, dimensional, inferential diagnostic system to a ‘neo-Kraepelinian’, descriptive, symptom-focused, multiaxial classification relying on present-versus-absent criteria sets for identifying discrete mental disorders” (PDM-2, 2017, p. 1).
This move away from understanding the person as a whole and, instead, looking at groups of symptoms as disorders, has caused a divide in mental health theory and treatment that has had a ripple effect in the mainstream field of psychotherapy around the world that still lasts to this day. Medical model theory has been taught in collegiate psychotherapy programs, separate from psychoanalytic theory and method. It also drove a quantitative symptom-focused label of the borderline personality, which practically wiped out the original use of the term founded in psychoanalytic tradition. However, many of us have experienced the resistance to viewing patients in terms of categorical labels:
“In the current era, they [clinicians] find themselves having to choose between reluctantly ‘accepting’ the DSM diagnostic labels, ‘denying’ them, or developing alternatives more consistent with the dimensional, inferential, contextual, biopsychosocial diagnostic formulations characteristic of psychoanalytic and humanistic approaches” (PDM-2).
The traditional Bioenergetic Analysis that I was taught was a theory and method for an alternative approach, but in the shadow of this medical model.
Many of us have, as licensed counselors, marriage and family therapists, psychologists, social workers, nurses, and doctors, come from medical model-based degree programs and, through the Bioenergetic Analysis branch of psychotherapy, stepped into the world of psychoanalysis and multi-dimensional assessment and diagnosis. With the symptom-focused background of whatever DSM or ICD coding system was in publication at the time of their schooling, trainees in Bioenergetic programs also learned the physiology, energy, character styles, transferences, and counter-transferences involved in working analytically, multidimensionally, and relationally. The two quite opposing viewpoints of “mental illness” collide in Bioenergetic training programs. If we follow the categorization of the Diagnostic and Statistical Manual (DSM), we miss integrating a critical theoretical piece that “suggest[s] a classification combining dynamic and structural explanations” (Kernberg 1976).
Personality Organization and Character Structure: Introduction
Through understanding the theory and concepts of Personality Organization I’ve come to believe the patients whom I mentioned in the first paragraph had defenses that were decompensating because their self-structure was not solidly organized. The Personality Organization template has explained the term “borderline” in a way that resolved the conflicts I had been reading about borderline personality disorder. Understanding the concept of borderline as a personality organization, and not as a syndrome, is a critical component of this theory.
What Personality Organization offers us is a perspective for building, or forming, a person’s self-structure. What Bioenergetic Analysis offers is the knowledge for when and how to challenge character defenses that no longer serve a person. If we integrate the two, therapists of our profession will have an even more multi-dimensional way of assessing and relating to the people who are our patients. This article will explain Personality Organization and its four levels and will define the psychoanalytic understanding and use of the term “borderline”. I will go on to compare and contrast Personality Organization and Character Structure theories and show how they can be integrated to form a holistic analytic theoretical model. Lastly, I will give an introductory overview of treatment considerations and how to work with borderline personality organization from a Bioenergetic approach. Let’s start with working definitions of self and self-structure so we have that conceptual foundation and move on to Personality Organization.
Defining Self and Self-Structure
Looking through a lens of self and self-structure allows us to view people as people and not as symptom clusters. The introduction of the PDM-2 states that “personality is more about who one is than about what disorder one has” (2017, p. 16). The concepts of the self and self-structure are foundational to the construct of Personality Organization. What constitutes the self has been examined philosophically, socially, psychologically, and psychoanalytically for hundreds of years, and in modern psychiatric and cognitive neuroscience at a fast pace in the past 30 years. For the purposes of this paper, I compile a general definition of self and self-structure from several modern sources, Bioenergetic Analysis, and modern neuroscience.
Dr. Dan Seigel, Clinical Professor of Psychiatry, and a man leading the charge for studying interpersonal neurobiology, proposes a definition of self by looking at the theory of mind. He states that “mind includes the self-organizing emergent embodied and relational process of that regulatory energy and information flow of relationships and body […] there’s no way to define the mind without going to energy.” He concludes by saying “the self then is not just a singular noun, it is a plural verb” (2011). Jonathon D. Brown describes observational factors of “I” and “me”. “I refer[s] to that aspect of self that is actively perceiving, thinking, or […] seeing” (1998, p. 5). The term me “refer[s] to that aspect of the self that is an object of our attention, thought, or perception. Self is both the seer and the seen, and the self has the reflective ability which we can call consciousness, self-awareness, or metacognition”. Antonio Damasio (2010, pp. 9ff.) says that the “me, the self-as-object (is) a dynamic collection of integrated neural processes, centered on the representation of the living body, that finds expression in a dynamic collection of integrated mental processes,” whereas the “I”, the “self-as-subject […] is a more elusive presence, far less collected in mental or biological terms than the me, more dispersed, often dissolved in the stream of consciousness, at times so annoyingly subtle that it is there is almost not there […]. When the brain manages to introduce a knower in the mind, subjectivity follows.” And lastly, Professor of Cognitive and Computational Neuroscience, Dr. Anil Seth, identifies five elements of the self: bodily self, perspectival self, volitional self, narrative self, and social self (Seth, 2021). In the perspectival, volitional, and social self we are being shaped by, and shaping our environment, including the people in it through the relation process Seigel describes. In summary, we can say that what we call our “self” is an ongoing energetic process of observing and being observed, impacting, and being impacted by others in the environment, through our bodily and perspectival self.
The self is so complex we cannot even observe the entirety of ourselves in any single moment. So, in turn, there is a narrative we create of ourselves that we use as the common thread strung through our experiences, that is informed by energy and (hopefully) a reality-based relationship to our environment. This is a major foundation of self-structure. Self-structure manifests in one’s cognitive and affective processes, one’s subjective sense of identity inside relationships, one’s stress resilience, one’s self-awareness, and one’s sense of meaning and purpose in life (their Personality Organization). The concept of self-structure, which the theory of personality organization rests upon, can be defined as the structure in which a person: (a) “has an internal awareness of oneself as unique, defined, and continuous person”; (b) “has that sustained awareness over time and in varying conditions”; and (c) “can relate that awareness of their self from both subjective and objective perspectives” (Scott Baum, personal communication, October 14, 2020). With this construct of the “self” we can move on to examine how the self is organized.
Character Structure and Four Levels of Personality Organization
Bioenergetic Analysis identifies five main character structures that correlate to the developmental stages from birth to approximately seven years of age: schizoid, oral, masochistic, psychopathic, and rigid. In her article “Borderline Character Structure Revisited,” Vincentia Schroeter (2009) proposes that “a person may be any character type, but within that type, operate at a low (psychotic) to middle (borderline) to higher (neurotic) level of functioning”. We can see that Personality Organization theory explains just that, and the PDM-2, gives definitions for four levels of self-organization: healthy, neurotic, borderline, and psychotic. Once we understand these four levels, we can then examine how this is compared to, and integrated with, the theory of character structure.
1) Healthy Level of Self Organization
Healthy organization is defined in PDM-2 as “people who become symptomatic under stress […] they may have certain favored ways of coping, but they have enough flexibility to accommodate adequately to challenging realities” (2017, p. 20). People with healthy organization usually don’t seek therapy, unless they are experiencing acute event trauma such as being in an accident, being diagnosed with cancer, or fighting in war. We see no other major traumas in their histories and note flexibility in their characterological patterns. They report symptoms limited to the event(s), joy in their life, and satisfying relationships. In this article I will not expand on the healthy structure, but will focus on the study of the other organizations.
2) Neurotic Level of Self Organization
The PDM-2 explains that “Individuals with neurotic-level personality organizations […] tend to respond to certain stresses with a relatively restricted range of defenses and coping strategies” (2017, p. 21). Looking through the Bioenergetic lens we can see that “restricted range of defenses” is a character structure. This level is where Character Analysis and the Bioenergetic method is very effective. We see patterns in a person’s history of ineffective coping or behaviors that lead them to feeling dissatisfied in life, and their self-reported dissatisfaction is what drives them to refer themselves for therapy. We can see abuse or neglect in family histories but also note the supports and coping abilities. We may also see a history of family tragedy such as loss of a family member, move in location, or addiction that impact their construct of the family. People neurotically organized can have long term relationships and stable careers or repeated patterns of failure in these areas.
3) Borderline Level of Self Organization
Note that the next level, Borderline, is separate from the concept of “Borderline Personality Disorder” as found in the DSM V. The history of how the term borderline came to be used as single, distinctive syndrome is part of the overall history of moving from a psychoanalytic to a medical model of diagnosis. Traditionally in psychoanalysis there were two ways of viewing a client: Neurotic versus Psychotic. In Psychoanalytic Diagnosis (2011, p. 52) McWilliams writes:
“By the middle 1950s, the mental health community had followed these innovators in noting the limitations of the neurosis-versus-psychosis model. Numerous analysts began complaining about clients who seemed character disordered, but in a peculiarly chaotic way. Because they rarely or never reported hallucinations or delusions, they could not be considered psychotic, but they also lacked the consistency of neurotic-level patients […] they were too sane to be considered crazy, and too crazy to be considered sane.”
People who are organized and function in a borderline way “have difficulties with affect regulation and are consequently vulnerable to extremes of overwhelming affect, including episodes of intense depression, anxiety, and rage. They may have recurrent relational difficulties; severe problems with emotional intimacy; problems with work, and problems with impulse regulation” (PDM-2, 2017, p. 21). Kernberg emphasizes that the use of primitive defenses, especially that of splitting and the absence of more mature defenses, as a key to the borderline organization (Kernberg, 2004). We see mixed patterns in their life of stability and breakdown that can take many different presentations. In one instance we can observe that they do very well in their career but have volatility and, perhaps, violence in their personal relationships. Or a second presentation could be that a person has periods in their life where they function very well in career and relationships, then periods where all areas break down at once – they lose their job and break off a relationship around the same time. A third presentation is that they arrive in our office well put-together and clear, seeking help for characterological issues, but reporting times in their histories of fractured relationships, job losses, a single psychotic episode, or substance abuse issues. We can often hear in the story of the person with borderline organization a history of abuse, addiction, or mentally ill parents. Family change or tragedy seems more intense or encompassing (both parents are abusive or neglectful as opposed to just one) than what we hear from those neurotically organized. Subjectively they experience confusion about their own contrasts, or complete absence of awareness that they become disorganized (depending on their capacity for self-observation).
4) Psychotic Level of Self Organization
In the same vein, the use of the term psychotic is not used as a term to denote a condition that afflicts a person such as schizophrenia, but the most underdeveloped way in which a person can organize their sense of self. As described in PDM-2, “[t]he psychotic level of personality organization implies identity diffusion, poor differentiation between representations of self and others, poor discrimination between fantasy and external reality, reliance on primitive defenses, and severe deficits in reality testing”. I will also include “overgeneralized, concrete or bizarre thinking” (PDM-2, 2017, p. 23). I am reminded of a client who called for an appointment five months after graduating with his bachelor’s degree, but was elusive about his treatment history, and chose to schedule out a month as he was taking a trip to Europe. His only observable symptom on the phone was monotone speech. Upon meeting him he was pleasant, sweet, quite focused on what he wanted from treatment (to make and keep friends), but he was self-absorbed to the point that he talked at me instead of with me, ignored my social cues, and had little patience or focus for my talking. He had a history of job losses, early discharge from the military, and no close friends, due to “outburst” behavior that he described as “tantrums”. His mother had mental illness, his father had rage episodes, and both appeared to have alcoholism. In session he seemed bothered by my reflections, and instead, stayed in his own train of thought. He hated the feel of his body to the point he would only bathe reluctantly and perseverated on the theme that he was a “piece of shit”. He explained that he had the sense his action figures could see, hear, and make judgements about him, which he called his “obsession”. He was an extremely talented artist. His legs from hip joints down reminded me of how a toddler’s legs are still slightly bowed and fatty and he had the traditional shoulder girdle tightness we see in Schizoid Character. Later I learned that he was notably irritable by the age of three and his social difficulties started around age nine when his peers moved into abstract thinking; he still presented with concrete operational thinking. His symptoms, cognitive functions, and behaviors met the DSM criteria for both Schizophrenia and Borderline Personality Disorder. In psychoanalytic terms he is psychotically organized with a schizoid character structure.
Personality Organization versus Character Structure
Personality Organization defines how we can observe a person’s capacity to perceive and interact with reality in a psychic way, and how one experiences their sense of self. In other words, and in the common language of the PDM-2, it’s the level of psychic or mental functioning with reality. Personality Organization is a way of understanding a person’s level of Mental Functioning in 12 areas or domains:
- Capacity for regulation of affect, attention, and learning
- Capacity for affective range, communication, and understanding
- Capacity for mentalization and self-reflective functioning
- Capacity for differentiation and integration (identity)
- Capacity for relationships and intimacy
- Capacity for self-esteem regulation and quality of internal experience
- Capacity for impulse control and regulation
- Capacity for defensive functioning
- Capacity for adaptation, resiliency, and strength (stress resilience)
- Self-observing capacities (psychological mindedness)
- Capacity to construct and use internal standards and ideals (morality)
- Capacity for meaning and purpose
Note: 1–3 relate to cognitive and affective processes; 4–6 relate to identity and relationships; 7–9 relate to defense and coping; and 10–12 relate to self-awareness and self-direction. PDM-2 (2017, p. 76).
We can assess a person within these 12 capacities and determine if they function healthily, neurotically, psychotically, or somewhere in between (borderline). The levels denote how a person both processes information about the world and how they subjectively experience their sense of self, i. e., how they experience themselves as a whole, congruous “I”. Character Structure is the style in which a person interacts with the reality of their world and those in it. Character Structure determines the themes of the internal and intimate conflicts one has, the relied upon personality pattern in which a person experiences their identity, engages in intimacy, and experiences their self-esteem, which is congruous to the pattern of managing impulses via the body’s energetic form.
To paint a picture of this we can think of a person with an Oral character who has a conflict between need and independence, their behavioral pattern of “exaggerated independence”, their relational clinginess, their self-esteem often having a collapsed or immature quality to it, with all this in a body that breathes shallow and has low energy or cycles between anxiety and depressed energy. Looking at all the people with Oral Character structure we can differentiate between those who have, for instance, the ability to imagine or mentalize what another is feeling, and those who cannot or are incorrect in what they determine about another. There are people who can observe the neediness in themselves when you point it out and feel self-compassion, and those who will struggle to comprehend what you are getting at because they get triggered (dysregulated) at an attempt to address their schema of themselves. We can therefore see both neurotically organized oral characters and those organized in a borderline way (I leave out psychotic here for simplification).
We can understand the difference between organization and structure through a self vs. other developmental lens. Personality Organization is an intrapsychic organization and is a window into the way a person processes information about the world and the way they experience themselves. Through studying attachment and neuroscience, I have come to believe that Personality Organization is formed in the early months of life as a child moves from autism to symbiosis with mother and through differentiation, when the infant’s nervous system regulation and interpersonal cueing is dependent on the primary caregivers’ responsiveness. Character structure is an interpersonal adaptation, that is behavior developed once differentiated, that is formed for a child first inside their initial primary triad with mom and dad, and next their family of origin. Character Structure serves to manage stress in the environment and is a strategy for maintaining connection with others. Personality Organization is the framework for how a person regulates one’s own individual self and is more about relationship to oneself.
The use of applied techniques is different for each framework. Using the knowledge of Character Structures, we know the difference between the sweet transference feelings we will experience with a person with Schizoid Character versus the inferior transference feelings we will experience with a person with Psychopathic Character. We can see the pattern they regularly resort to, in order to maintain self-esteem, e. g., dissociate from feelings or maintain an inflated stance. Using the knowledge of Personality Organization, we can determine if a person has enough internal, sustained awareness to tolerate the direct reflection of a dynamic that needs to be brought to consciousness, or if they need an intervention that requires building a reflective capacity that increases self-structure. This is the difference between saying “you hate that he’s above you” versus “it seems you have strong negative feelings about what’s going on”. In the first reflection it is assumed that the person can observe that you are a separate person giving your interpretation. It is a convergent idea, and they could agree or disagree with you. In the latter reflection you are modeling curiosity and observation in a divergent way, so that they can be open and explore.
Schroeter (2009) reflects on Horner’s schema that “borderline fails to create a cohesive individuated self”. This highlights a “pathology of self-structure” that contrasts with the developmental model of character structure. When we are considering borderline or psychotic organization, we are looking at damage to self, not adaptation to environment. In character structure we are looking at developmental adaptations that no longer serve a person. There is a difference between failures of development that lead to adaptations and the mangling of development that leads to incapacities. The immune system of a mother who is Rh-negative will send antibodies to destroy the red blood cells of her Rh-positive baby. The baby fails to maintain enough red blood cells not because of a failure in development of those red blood cells, but because of pathological incompatibility that destroys what is formed.
Using these two theories we can understand a person from 2 different angles. We can use Personality Organization to discern a patient’s overall congruent reality, prognosed length of time needed in treatment, expected course of treatment, realistic goals, boundaries of treatment, and what level of relational interaction is possible and needed. Understanding Character Structure and Bioenergetic method a therapist can determine what techniques will best move the energy, increase sensation, and open feeling for a person to illuminate a sense and understanding of their unconscious motives and defenses.
A Word on Defense Mechanisms: Primitive and Secondary
The 8th capacity of the PDM-2 is to evaluate the patient’s capacity for defensive functioning. Examining which types of defense a patient uses can be a guide for a therapist to determine the level of personality organization. This article is limited to mentioning the defenses and not explicating them, so this writer encourages the reader to undertake their own study. What we can identify here is that defense mechanisms relate to how a person functions in their own awareness of themselves, and their ability to observe and adjust to reality. Note that defense mechanisms are used under stress. “Primitive defenses operate in a global, undifferentiated way in a person’s total sensorium, fusing cognitive, affective, and behavioral dimensions, whereas more advanced ones make specific transformations of thought, feeling, sensation, or behavior, or some combination of these” (McWilliams, 2011, p. 102). Primary, or primitive defenses, include withdrawal/isolation, denial, omnipotent control, idealization/devaluation, projection, introjection, projective identification, splitting, somatization, defensive enactment, sexualization, and dissociation in extreme forms such as catatonia. Secondary defenses, or the defenses that indicate more neurotic level of functioning include repression, regression, isolation of affect, intellectualization, rationalization, moralization, compartmentalization, undoing, turning against the self, displacement, reaction formation, reversal, identification, sublimation, and my favorite, humor. As we assess our clients and create hypotheses, we can look to the defense mechanisms, if personality organization is not easily deduced from their history or felt in countertransference. All character structures can use all defense mechanisms.
A Circumplex Model That Integrates
We can integrate the functional understanding provided by the PDM-2 (e. g., the four levels of Personality Organization and the 12 categories of Mental Functioning) with the Bioenergetic Character Structures using a circumplex model1. In our mind’s eye we can place the Character Structures on a horizontal line, with Schizoid at the left end and Rigid on the right. This gives a mental picture to the developmental age of trauma or object relations failure. We can then place Personality Organization on a vertical line with healthy on the top and psychotic on the bottom. With the lines creating a cross we can draw a circle around them we now see quadrants (Figure 1). What we are assessing within the same circle is both development and pathology. These quadrants are not meant to label, but to hone the focus of understanding when assessing patients.
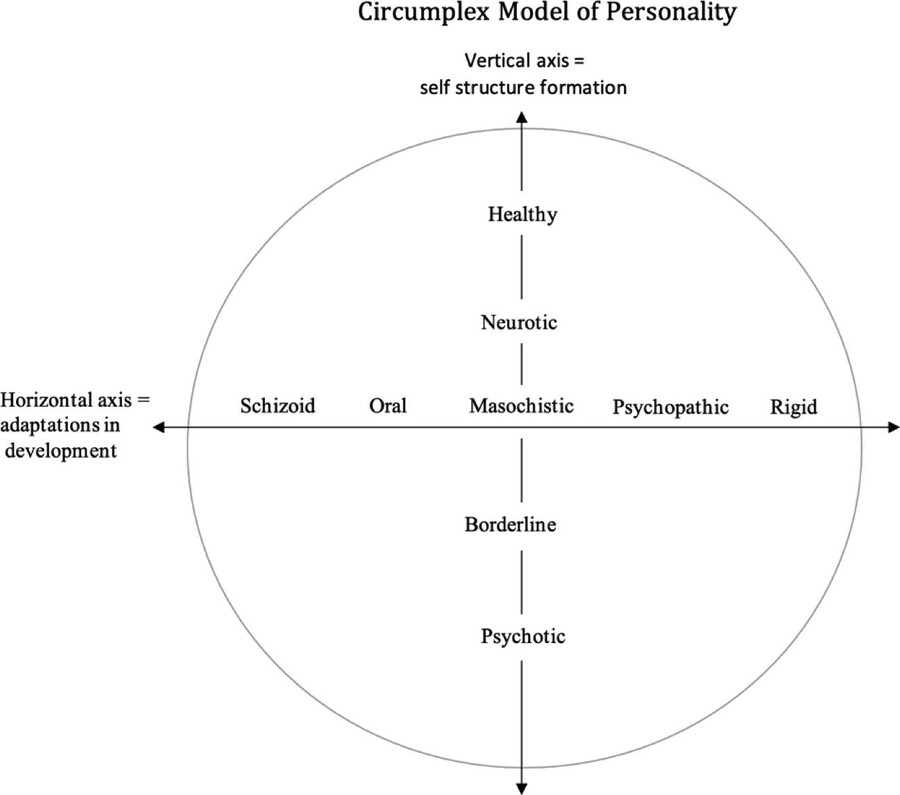
Figure 1. Circumplex Model of Personality (A. Coleman).
If we assess that someone falls in the upper right quadrant of the circle, we are looking at a neurotic to healthy with post-genital conflicts. We can move forward in the clinical relationship knowing they can integrate cathartic experiences from more challenging energetic techniques. If we assess that someone falls more in the lower left quadrant, we can know that we must proceed more slowly and carefully and seek to understand what their capacities and limitations are before we attempt cathartic exercises. Simply put, we can have more clarity in planning and creating effective therapeutic interventions. We can decide between something like grounding vs expression. This is not to say that those with neurotic organizations can bypass grounding or awareness building. I am saying that, in my experience, those with borderline and psychotic organizations must have grounding and awareness before a cathartic experience can have a positive therapeutic impact, and that this may take years to accomplish.
Naturally this model does not account for wants, desires, humor, impactful events, musical preference, hopes, dream, and the myriad of other things that makes a person their own unique self to which we connect. Keeping in mind the multi-dimensional and inferential approach, we can see that, much like the sense of self, we as clinicians cannot see and take into account all aspects of a patient at once. This model allows us to hold two aspects at the same time. I believe this model simply creates points of focus and clears the mystery when we see so many variables and are deciding our clinical approach. A person with a primary oral character structure that functions at a neurotic level behaves, and has an internal experience, much different than someone with oral character structure that functions at the psychotic level. What I seek to highlight is that these two people require different clinical approaches depending on their capacities of self-observation, identity, mentalization, etc. As Bioenergetic Therapists this clarity informs, but does not replace, our ability to work in the present with energy and in relationship with the client.
Variances of Personality Organization
To paint the picture of what is seen with the circumplex model we will take one character structure and view examples of how that person would present at three of the levels of personality organization. First, let’s look at an example of a person with masochistic character structure responding to an interpersonal conflict inside a job role.
Neurotic Masochism
We can begin by imagining a person with masochist character structure, who is neurotically organized, who is criticized by a boss to whom they feel loyal. We can expect that they are going to rely on maneuvers of trying harder to please their boss instead of facing conflict head on, rationalizing, moralizing, and complaining in an ego-syntonic attempt to ground. Their perspective would be rooted in accepting the suffering they are in, while, perhaps, engaging in a passive-aggressive action. We can energetically feel their bind as a pressure or a vice. We can view the behavior as their ineffective pattern of self-defeat. Their strategy does not bring them agency or true connection or satisfying relational repair, but nonetheless it is a strategy that is experienced as a continuous, defined, sense of self. If you, as clinician, reflected your objective perspective, their subjective experience would line up to a reliable degree. A direct reflection would work because the person has an observing ego.
Borderline Masochism
A person with a masochistic character style that is organized in a borderline way and is criticized by a boss to whom they feel loyal will have less of a strategy and will not function as well. We sometimes call this being “triggered”. They may become confused (less ability to mentalize) and irate (dysregulated). We may observe their shock/surprise and may hear them tell us of inappropriate attempts to seek other’s (including the therapist’s) opinions so that they have an “authority” making sense of this for them. Seeking other authority can be an indication of the lack of a central narrative thread. They may rely on splitting and devaluing the boss into an all-bad being. We may viscerally feel chaos or sleepiness as an energetic transference. They have temporarily lost their strategy because their perceptual and narrative self has become disorganized. The sense of self and the past experiences with it, can disappear so that their experience is one of stimulating, fast moving sensory information with no historical reference for organizing information. This usually functional person has slid away from neuroticism and towards the more psychotic end of personality functioning under the stressful situation of interpersonal conflict. This person may not be able to process a direct reflection because the congruence of self-structure is fractured in the moment and self-reflection is limited. It’s important to note that the characterological pattern we see from their physical build, which manifests in personality, can be a defensive structure that organizes a disorganized experience. If you observe this person using their characterological defense, they are organizing themselves. “Well, I just won’t tell him when I complete his list, he can figure it out for himself!” is a masochistic style relational response to mis-attunement, and we may see them come to this position as they reorganize themselves inside our office. In this example this person has lost their consistent neurotic pattern but is not fully delusional.
Psychotic Masochism
For the person who has a psychotic organization, with a masochistic character style, and is criticized by a boss, we can first say that we may not even see a sense of loyalty as we usually would just looking at character style. They may not have a construct of loyalty inside a relationship, but instead what could be called loyalty presents as a rigid routine of being to work on time every day, as the behavioral habit creates a structure. Their day-to-day experience of life is that of just trying to get by, and we may see them spending their energy simply trying to create a construct for what is happening with the boss who criticized them. We may see emotional upset/agitation, a dysregulation episode, and/or a delusional narrative. We will see more primary defense mechanisms and, understanding that this person characterologically has masochism, we may see a narrative take the theme of sadism or suffering: “I’ve done badly, and I must eat shit”. I’m reminded of one man I met in a psychiatric setting who frequently attempted to eat garbage out of dumpsters to punish himself the way his mother punished him as a child. It is unlikely that we will see our client empathize with the boss’s point of view. They will likely seek a concrete solution to their confusion. The resolution they seek is not interpersonal, it is intrapersonal in terms of them simply finding some way, likely ineffectively, to view, feel, and ground in reality.
Treatment Considerations
The next step after understanding the circumplex model is applying it to practice. Here I explain some general concepts, comparing and contrasting approaches to working with neurotic, borderline, and psychotic Personality Organization and Character Structure. When working with borderline or psychotic organizations we are working to build self-structure. When working with neurotic organization we work to illuminate characterological defenses.
Self-Forming vs. Characterological Challenge
The profound contribution Bioenergetic Analysis makes to psychoanalysis overall is the ability to work with the energy that forms impulses, emotions, volition, etc. and this also makes BA ideal for working with psychotic and borderline organization. However, it is important to determine when a self-building intervention is needed and when a character challenging approach is appropriate. What I am calling self-building means working on increasing the functioning of any, or all, of the 12 mental functioning capacities. Bioenergetic therapy can raise a person’s awareness and increase sensory feeling either in terms of capacity or their characterological style & self-defeating patterns. We do this through grounding, and charge and discharge. We often challenge character defenses so that a person can gain access to their authentic impulses and emotions. We might ask someone with oral character to reach so that they get in touch with the pain of not having fulfillment of their reach. Therapy with a person organized in a borderline or psychotic way involves forming a congruent, sustained, and aware sense of oneself. We can work on dynamics such as a person’s ability to observe themselves, or their ability to observe you as a separate person with potentially different thoughts and feelings. In this way body work can involve gentle, slow, forming work where the felt body sense and authentic impulses become the basis for increasing self-structure functioning. Also, in working this way, we do not assume security in the therapeutic relationship, we focus on building that security, usually slowly.
With those who are organized in a more neurotic way we can choose more stressful and challenging positions and movements such as the breathing stool, racket hitting, or physically close hands-on work that increases sensation quickly and transcends a characterological defense. Use of the breathing stool, for example, with someone with a rigid character can challenge their separation of heart and pelvis. When the neurotically organized person has a strong physical sensation, psychic sense (such as a feeling like mom is watching), or emotion come up, their intact self-structure allows them to compare this new experience with what they have been experiencing or believing historically. They also have a stronger tolerance for sudden or intense increases in charge and discharge and can make meaning of these changes. We can assess that when a person with neurotic organization is hitting a racket and suddenly bursts into tears, that their aggression has discharged sufficiently for them to access the vulnerable feelings they were defending against. And we know that this experience is a catharsis that can lead to transformation as they process the therapeutic moment through their knowing of who and what they are. A memory that returns or a sense of being abandoned, for example, can fit into a paradigm of themselves and their life.
In contrast, therapy with a person organized in the borderline or psychotic way aims at forming that ability to observe and create a reality-based narrative in relation to impulses and emotions that leads to a lasting self-structure. This includes building the ability to feel the body and make sense of the sensations and emotions, often in contrast to a concrete black-or-white narrative of themselves or their world. Developing self-structure includes developing primary defense mechanisms into secondary ones. If a person has borderline organization, it’s important to work with self-building through observational activities and relational work in the clinical holding environment before challenging their character structure.
No amount of grounding or body work alone will increase functioning, joy, or self-possession of someone with borderline organization. Connection to self is not a result of bodywork with someone with these organizations because the self is fleeting at best, and unrecognizable at worst. There is not much to which sensation can be attached; sensation is likely to be overwhelming or confusing. The lasting narrative thread on which to reflect and glean information from is not there. Safety and trust in the relational environment precede peace, ease, and joy. With these levels, increasing the ability to feel and assign reality-based meaning to what is happening in their body is of first priority, if a clinician determines body work to be helpful. This is done with exercises that include very basic grounding that moves into identifying sensation, reflecting, and framing meaning, exploring, and mirroring. Note the two latter can be relational techniques. Having a person identify what they feel on the inside and take in the reflection of what the clinician sees on the outside, is a technique that helps form one’s sense of self. The value of bioenergetic grounding exercises, such as the bow, can be used to assist a person in increase self-reflective functioning and practice creating meaning. Relational somatic activities allow mirroring that can be structured, slow, and temporary in which the person can relate to the therapist as a separate object. (The use of the term object is that of object relations theory).
In treatment, to attempt to illuminate a character style of someone psychotically organized, is like speaking Spanish to a German toddler – the abstract concepts don’t have any meaning and have no way to assimilate into a known experience; your facial expressions, tone, energy, boundaries, and mood are what they are able to observe, if & when they can observe, as they learn about the constancy of you. A simple, reality based meaning a psychotic patient could make from body work is “I can feel tension in my shoulders” or “that ball feels different to this ball”. This is profound for a person forming a self-structure. If their perception is accurate, each simple awareness becomes a grounded piece of narrative thread upon which they can build their sense of charge, discharge, like, dislike, pleasure, or unpleasure, and in turn, their sense of self.
We can, in those who have borderline organization, illuminate and work with their character structure in the process of building self-structure. With a person organized in a borderline way, therapy can often involve a dance between the self-forming and character challenging approaches, depending on the state your patient presents on the day you meet with them. When stress is low, they are likely to tolerate the change of sensation in grounding and characterological challenge; when particular stress is high, they are likely to decompensate and need to be brought back to self-observing and reorganizing strategies. Often the course of therapy includes more self-structure building in the first years of treatment moving towards strong, emotionally expressive, challenging work as time goes on. When a client has had a disorganizing episode, but are presenting organized in the treatment office, they need self-observing capacity to understand what happened for them. They came undone because … (you are filling in that blank together).
Case Example of Working with Borderline Organization
Misty is a sis-gender identified Caucasian woman in her early 30’s, married to a man, with one birth child of their unplanned pregnancy. She has a history of substance addiction and is in sustained recovery. She is highly intelligent and a quick learner with a history of impulsivity leading to job hopping. She has difficulty relating to others in group settings and has a history of intense friendships that lead to conflict and sudden break up, with her completely devaluing the other, or completely devaluing herself. Her mother had manic episodes and delusional ideas and Misty experienced physical, emotional, and mental abuse (gaslighting) as a child from her mother. Her father was experienced as “deadpan”, “gone tinkering in his own hobbies”, and “not there”, unable to mediate the abuse mother inflicted. She presents very well-articulated, put together, cogent but with tangential speech in the therapy office, and without a sense of what she is supposed to do with her life. She has a main rigid character structure of the sinuous type, secondary schizoid, with OCD tendencies. When discussing her need for a perfectly clean house we explore this in terms of her character traits and as an attempt to manage generalized anxiety that people with diffuse self-structure often feel on a daily basis. She can identify how keeping the house clean exhausts her, but having an unclean house keeps her anxious – a manifestation of disintegrated opposites (all clean or all dirty) that is a marker of the split sense of self indicative of some borderline organized experience. She is able to discuss her conflicts of not wanting sex both in terms of a heart and pelvis disconnect, and a single event rape she experienced as a young adult. Many times she has come to session highly anxious, shaky, and confused (in what I call residual shock), explaining a fight with her mother-in-law or girls at her work.
Early in working with her she presented with tangential thinking and in symbiosis with me as an object – she talked at me non-stop. I realized that she appeared threatened by and would shirk away from anything I did or said that asked her to interact with me as a separate other. She spoke to her fear of the somatic work and stayed stiffly seated in the same spot each session. She did not understand the reason for all the conflictual relationships in her life but felt the pain of repeated relational disintegrations. I imagined she was pretty scared this pattern could be repeated with me, and I could feel her tortured conflict in wanting to know me vs. needing to use me as an object. Her diffuse sense of self meant she was at risk of merging with me. In addition, her internalized model of interpersonal relations was to use or be used, and to either please or displease authority. This meant that she was vigilant in examining my movements and facial cues and became anxious when I kept a straight face. One day when sharing her pain with me I asked her to look at my face and imagine what I might be feeling. She shook her head slowly and expressed that she couldn’t tell. I told her I was feeling compassion for her pain and fondness (I know that I was smiling) for her tenacious spirit to which she replied, “I can’t read that at all”. From that point we did what I call face-gazing work, where we would simply “talk” with our faces, mimicking how an infant and mother might volley expressions. I pointed out when we felt similar and when we felt different. This was a treatment born from Bioenergetic method but based in the theory of Personality Organization. It meant she could stay seated right where she was as she built the capacity for mentalization and psychological mindedness.
In one instance, about 3 years into treatment, she came to session appearing distressed, twitching, teary, and reported that her mother-in-law had criticized her for not allowing the mother-in-law (a college mathematician) to tutor her daughter. She could not organize her rationale for saying no in the moment, but instead, she presented feeling dazed, angry, and confused while behaving appalled and preoccupied with her mother-in-law. It seemed clear that her self-structure fracture and inner panic was covered by outward anger. Her congruous sense of self was temporarily disorganized; she had no awareness of what thread was the foundation of the fabric of her Self. She labeled her mother-in-law as a “narcissistic control-freak”. I asked her to observe what she was physically feeling and where. This brought her to both 1) the recognition of a familiar feeling behind her sternum, and an unexplainable pain in her knee, and 2) awareness of the difficulty feeling anything else. Her perceptual and bodily experience was compromised, but something was still there (and it didn’t make sense). I asked what she saw in my face as she told the story. She accurately read wincing pain and concern in my face (the mother-in-law is quite belittling and cruel). Modeling my observing ego and offering my reality testing I reflected my view of what I heard in her story, that her mother-in-law was behaving in a self-serving manner under the guise that it was good for her daughter (a gaslighting maneuver of mental abuse) and resorted to punishment tactics in order to get my client to change her mind. This interpretation soothed and calmed her. She expressed “I mean she’s amazing at math, but she doesn’t understand what a kid like mine needs”. She began to re-organize her rationale. As we talked, she found validation of what she sensed was a reality, but in an integrated way as her mother-in-law was not an all good or all bad being.
The therapeutic application was to have her observe her internal emotional and body experience, offer her an objective observation from the outside, and have her begin to reconstruct her sense of self with observation of these two perceptual perspectives. She was able to then recall why she said “no”, which was based on her knowledge that her mother-in-law had historically not been able to manage her daughter’s ADHD behaviors and would take punitive action, which she did not agree with. Not treating a child punitively was part of her values and narrative self-structure thread. She moved to feeling positive and certain about her decision, and a sense of herself as being a worthwhile parent with clear and valid values. I reflected my observation that she seemed clear and sure, which she reported she felt on the inside. Her inner reality now matched her outward behavior; I was the mirror. I then invited her to move as she saw fit, and she stretched in a natural way that was based on her own impulse, and in a way that indicated to me ANS regulation. We discussed the potential meaning of the pain in her knee, and although she could not make meaning of it, she indicated she could tolerate not knowing what it meant. Note that talk from a psychoanalytic perspective, for the purpose of regulating and establishing a reality base, preceded body work that supported what she now sensed about herself. Also note, that her primary defenses of devaluation and somatization changed to rationalization, a secondary defense, and moved towards tolerating the unknown, an action of self-structure. The next step for a future session, as determined by Misty, was to work on what boundaries she wanted to establish with her mother-in-law to prevent another degrading attack. We must have some sense that we are a separate, unique, and continuous person in order to want to work on our boundaries with others.
Conclusion
Medical model mental health education and experience does not teach us how to understand people with severe mental health disorders or severe abuse and neglect histories. Training in Bioenergetic Analysis opens the door to knowing there is so much more. Remember that BA is born from psychoanalysis. The limitation of the medical model of classifying disorders has created a diversion that has prevented us as bioenergetic therapists from understanding a full model of assessment. Especially the idea that “borderline” is a discrete disorder. We must look at a person and how they experience their sense of self. If we turn to look at the whole of psychoanalytic contributions, we can combine the theory and somatic treatment techniques of Character Analysis with the structural understanding of Personality Organization. This allows us to provide a comprehensive holistic approach to treating those with borderline and psychotic organizations. What Personality Organization offers us is a perspective for building, or forming, a person’s self-structure. What Bioenergetic Analysis offers is the knowledge for when and how to challenge characterological defenses that no longer serve a person. Personality Organization and Character Structure inform one another and can be used together to create a holistic approach to long term treatment.
This article is limited to comparing and contrasting the two theoretical approaches and demonstrating how they complement one another. A circumplex model illustrates this nicely. What comes next is using our knowledge and repertoire of somatic techniques to treat those with borderline and psychotic organization. How do we create techniques that help develop a person’s capacity for self-awareness? Or integration of a differentiated identity? Or mentalization? This is an exciting study in which the field of Bioenergetic Analysis, and the inclusion of the body, plays an important role.
References
Brown, J. D. (1998). The self. New York: Psychology Press.
Damasio, A. (2010). Self comes to mind: Constructing the conscious brain. New York: Pantheon Books.
Freud, S. (1991). On narcissism: An introduction. Yale Uni Press.
Kernberg, O. (1976). Object-relations theory and clinical psychoanalysis. New York: Jason Aronson.
Kernberg, O. (2004). Borderline conditions and pathological narcissism. Lanham, MD: Rowman & Littlefield.
Lingiardi, V., & Mc Williams, N. (Eds.). Psychodynamic Diagnostic Manual: Second Edition, PDM-2. New York, London: Guildford Press.
McWilliams, N. (2011). Psychoanalytic diagnosis: Understanding personality structure in the clinical process (2nd ed.). New York, London: Guildford Press.
Mitchell, S. A., and Black, M. J. (2016). Freud and beyond: A history of modern psychoanalytic thought. New York: Basic Books.
Ohio State University. (2013). History of DSM, Nov. 2013, tpb.psy.ohio state.edu/5681/notes/ dsm/01.htm
PDM Task Force. (2006). Psychodynamic Diagnostic Manual. Silver Spring, MD: Alliance of Psychoanalytic Organizations.
Reich, W. (1972). Character analysis. New York: Farrar, Straus, & Giroux.
Seigel, D. (2011). Keynote address. Presented at 21st International Institute for Bioenergetic Analysis (IIBA) conference, San Diego.
Seth, A. (2021). Being you: A new science of consciousness. Penguin Random House.
Schroeter, V. (2009). Borderline character structure revisited. Bioenergetic Analysis, (19), 31–52.
The author
Ann Coleman, LMSW, CBT, is a former IIBA board member and former treasurer for NANZIBA. She is a clinical social worker in private practice in metro Detroit Michigan. Ann is currently an assistant trainer working towards local trainer status with the Massachusetts Society training program, and has facilitated many educational workshops at North American conferences. Her perspective is drawn from years of work in juvenile detention and psychiatric systems that served people with severe and persistent mental illness. She has a special affinity for addiction recovery and it’s co-occurrence with mental illness.
Anmerkung
- [1]
- A circumplex model is a diagram that allows the viewer to examine the interaction of two or more dimensions and to draw intuitive inferences from that interaction.