Lesbians, Gay Men, Bisexuals, Trans, Inter and Queers*
Some challenges for the theory and work of Bioenergetic Therapists1
Thomas Heinrich
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2019 (29), 57–78
https://doi.org/10.30820/0743-4804-2019-29-57 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstracts
Since the International Conference of the IIBA in 2007 at Sevilla, the shift of attitude in the Bioenergetic world towards LGB* to an affirmative one became public. Simultaneously, in the Bioenergetic world the publishing on this topic stopped. The resulting gap to the meanwhile increased knowledge of LGBTIQ* affirmative research will hereby filled up by information about the life situation of LGBTIQ*, an empathetic change of perspective on the LGBTIQ* world and some considerations on a Bioenergetic affirmative approach for the body related psychotherapy with LGBTIQ* clients.
Key words: biological sex, gender identity, sexual orientation, sex role, trans*.
Lesbiennes, Homosexuels, Bisexuels, Trans, Inter et “Queers”*. Quelques Défis pour la Théorie et le Travail en Analyse Bioénergétique (French)
Un changement d’attitude envers les LHB* (Lesbiennes, Homosexuels et Bisexuels) s’est affirmé publiquement depuis la conférence internationale de l’IIBA en 2017 à Séville. Mais, simultanément, les publications sur ce sujet dans le monde bioénergétique ont cessé. Le but de cet article est de combler la distance en termes de connaissances engrangée sur la recherche d’affirmation des LHBTIQ en donnant des informations sur la situation de vie des LHBTIQ*: un changement de perspective empathique vis-à-vis du monde LHBITQ* et quelques considérations sur l’approche bioénergétique affirmative en psychothérapie corporelle pour les clients LHBITQ*.
Lesbianas, Hombres Gays, Bisexuales, Trans, Inter y Queers*. Algunos Desafíos para la Teoría y el Trabajo de los Terapeutas Bioenergeticos (Spanish)
Desde la conferencia internacional del IIBA en Sevilla, 2007, el cambio de actitud en el mundo de la bioenergética en relación a los LGB* fue de tono afirmativo, y hecho público. Simultaneamente, en el mismo mundo bioenergético, las publicaciones con éste tópico cesaron. La brecha resultante del momentáneo incremento del conocimiento de las investigaciones afirmativas sobre LGBTIQ* serán llenadas por la información acerca de la situación de vida de los LSBTIQ*, un empático cambio de perspectiva sobre el mundo de los LGBTIQ* y algunas consideraciones sobre una aproximación bioenergética afirmativa hacia el cuerpo en relación a lá psicoterapia con clientes LGBTIQ*.
Lesbiche, Gay, Bisessuali, Trans, Inter e Queer*. Alcune Sfide per la Teoria e il Lavoro dei Terapeuti Bioenergetici (Italian)
A partire dalla conferenza internazionale dell’IIBA del 2007 a Siviglia, il cambiamento in positivo dell’atteggiamento del mondo bioenergetico nei confronti della LGB* è diventato pubblico. Contemporaneamente, nel mondo bioenergetico non ci sono più state pubblicazioni su questo argomento. Il divario che ne è risultato, mentre nel frattempo aumenta la conoscenza della ricerca affermativa LGBTIQ*, verrà colmato grazie a informazioni sulle condizioni di vita delle persone LSBTIQ*, il cambiamento di prospettiva empatico sul mondo LGBTIQ * e alcune considerazioni su un approccio affermativo bioenergetico per la psicoterapia corporea con Clienti LGBTIQ*.
Lésbicas, Gays, Bissexuais, Trans, Inter e “Queers”*. Alguns Desafios para a Teoria e Prática de Terapeutas Bioenergéticos (Portuguese)
Desde o congresso internacional do IIBA, em 2007, em Sevilha, a mudança para uma atitude afirmativa da Bioenergética em relação aos LGB*, tornou-se pública. Na mesma época, porém, as publicações sobre esse tópico, na área da Bioenergética cessaram. A lacuna resultante, considerando o conhecimento crescente de pesquisas afirmativas sobre LGBTIQ*, será preenchida pela informação sobre a situação de vida dos LGBTIQ*, pela mudança da perspectiva empática sobre o mundo LGBTIQ* e por algumas considerações a partir de uma abordagem bioenergética afirmativa com relação ao corpo, na psicoterapia com clientes LGBTIQ*.
Лесбиянки, геи, бисексуалы, транссексуалы, интерсексуалы и другие люди, чьи представления о сексуальной и половой принадлежности не соответствуют гетеросексуальным (далее по тексту используется аббревиатура LGBTIQ* (Russian)
После Международной конференции IIBA в 2007 году в Севилье стало известно, что отношение мира биоэнергетики к LGB* (геям, лесбиянкам, бисексуалам) изменилось в положительную сторону. В то же самое время публикации на эту тему в мире биоэнергетики прекратились. В этот период не поступало данных, касающихся LGBTIQ*, из каких-либо подтвержденных исследований. Однако этот пробел в ныне растущих знаниях о LGBTIQ* был заполнен благодаря поступающей информации о жизненных ситуациях LGBTIQ*, благодаря эмпатическому изменению взгляда на LGBTIQ* мир и также благодаря ряду разработок в области позитивного биоэнергетического подхода к телесной психотерапии у LGBTIQ* клиентов.
Introduction
As a gay man I was in a dilemma at the start of my psychotherapeutic training. On the one hand I was totally convinced of Bioenergetic theory built upon Wilhelm Reich’s research and Alexander Lowen’s further development, but on the other hand I experienced a total discrimination against non-heterosexual sexualities in their theories (Lowen, 1965).
At the same period, I became a member of the VLSP, the German branch of the ALGP, the Association of Lesbian and Gay Psychologists. There was an intensive discussion of affirmative research and approaches to psychotherapy with lesbians and gay men, starting with Hooker’s work (1957) which led to the cancellation of homosexuality as a disease in the DSM of the American Psychiatric Association in 1973, against the resistance of the American Psychoanalytic Association. The VLSP became a reservoir of support for me. Subsequently my colleagues and I established a psychiatric project for the work with gay men (Heinrich & Biechele, 2006; Biechele, Hammelstein & Heinrich, 2006).
I realized that Reich’s and Lowen’s attitude, especially to gay life and sexuality, was similar to the attitude of the psychoanalysts of the second generation. Rado (1940) criticized Freud’s thesis of a natural bisexuality and accepted only heterosexuality as natural. Socarides (1968) elaborated Rado’s theses even more precisely by devaluing all kind of non-heterosexual lives. Therefore, I concluded that perhaps Lowen should question his written statements devaluing non-heterosexual lives, which were, after all, not the keystone of his work. I subsequently applied for the training in Bioenergetic Analysis and experienced openness and welcome at first glance. At second glance I realized a lack of knowledge and hidden prejudices which in the best case were made explicit.
After my training I tried to open the discussion of Bioenergetic work for gay men and lesbians, by founding PLUS, the psychological counseling center for Lesbians and Gay men, with colleagues in 1999, in the region of the rivers Rhein and Neckar in Southern Germany. At the International Conference of the IIBA in 2005 at Cape Code, USA, I presented a paper entitled, Lesbians, Gay Men and Bisexuals – Bioenergetics with Unknown Species. I realized that there was another presenter with a very similar topic, and I had the great pleasure to make the acquaintance of Louise Frechette from Canada and her Bioenergetic work with lesbians and gay men.
At the following International Conference of the IIBA 2007 in Sevilla I experienced my most important morning in the international Bioenergetic World yet, when Garry Cockburn told the whole auditory that we could not follow Lowen’s statement, When I die, do not kill me! Garry told us, that we had to do this to find our own way in Bioenergetics, just as Lowen had done with his psychotherapeutic father Wilhelm Reich in order to find his own identity (Cockburn, 2008). His paper was followed by Scott Baum’s paper about the difficult relationship and the process to leave the shadow of the father (Baum, 2008). The next panelist was Fina Pla, from Spain, who presented a paper about a feminist approach to Bioenergetics contradicting Lowen’s patriarchal statements on women, followed by Paul Sussman, from the USA, who presented the results of a study about the situation of gay men which especially emphasized the necessity of being accepted by their families after they have informed them about their homosexual orientation.
Finally, I felt at home in the Bioenergetic world even as a gay man. Over time I got to know more and more gay, lesbian and bisexual Bioenergetic colleagues all over the world at the International Conferences of the IIBA. The Southern German Society for Bioenergetic Analysis even included a workshop about the Bioenergetic work with lesbian, gay and bisexual clients into their upcoming trainings.
All right. Right?
At the International Conference of the IIBA in Porto de Galinhas, Brazil, in 2015 I talked to some gay colleagues about the development in the Bioenergetic world of the LGBTIQ* issue and how modern Bioenergetic Analysis has taken this point into account. They answered that they still have experienced an underlying prejudice against non-heterosexual lives and that Lowen’s ancient quotes could still be part of some trainings. I was quite surprised by this news and wondered how this could be changed?
The most helpful idea seemed to me to follow the research on attitudes. Attitudes are pretty stable. It is not enough to present new information about a disputable issue. More than that, taking charge of another one’s view is needed as well as the training of new courses of action to change one’s attitude profoundly (Heinrich & Kohn, 2006). The following question then arose for me: How could a trainer for Bioenergetic Analysis include affirmative attitudes about LGBTIQ* lives in the training, if nothing about this issue had been published during the last 10 years, and only marginally beforehand?
When I read about the theme of the International Conference of the IIBA of 2017 in Toronto with one of its focal points on sexuality and community, I took the opportunity and sent in a paper for a workshop on Lesbians, gay men, bisexuals, trans and queers* – some challenges for the theory and work of Bioenergetic Therapists.
This article is following the three requirements to change attitudes:
- Information about the lives and the special situation of LGBTIQ*
- Possibilities to adopt the points of view of LGBTIQ*
- New courses of actions in Bioenergetic Analysis with LGBTIQ* clients.
The article might to be difficult to read in some parts. It might look like as a dictionary or a glossary. But stepping into a new continent of the human world, normally needs the openness to a new culture and the preparation of learning a new language.
Experiment
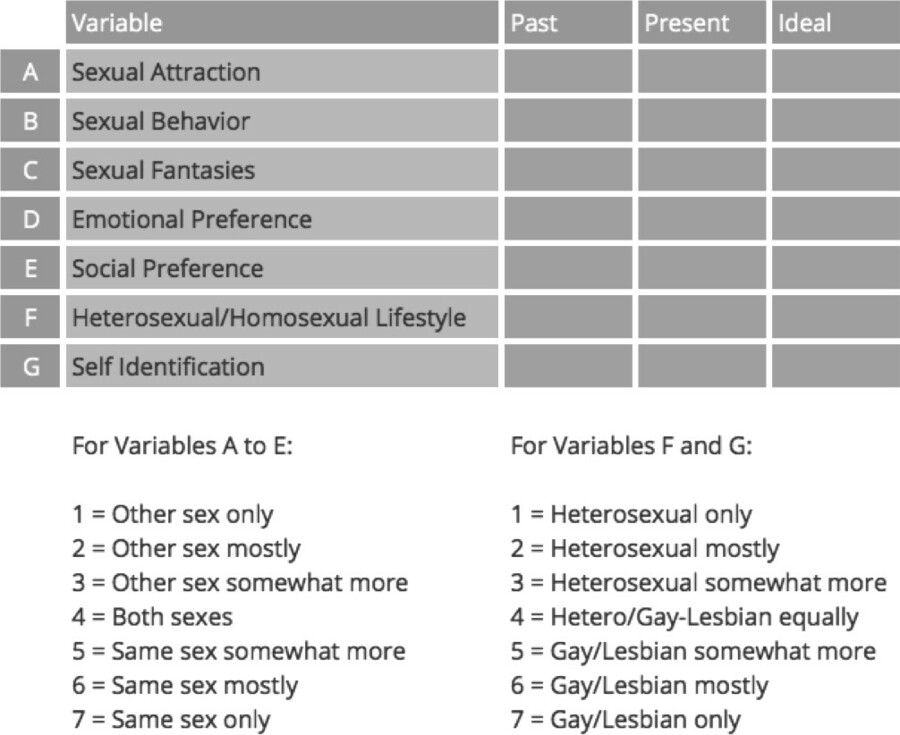
Klein’s Sexual Orientation Grid (1985, 1993)
The grid is constructed by Fritz Klein et al. in 1985 as a further development of Kinsey’s scale. It can be used as a first reflection on one’s own non-heterosexual aspects of one’s own personality. The following questions could help: How was it, to answer or even read the questions? Was there an emotional reaction in me, when I understood, what kind of information I have been asked? Did I feel ashamed or trapped? Was there another emotion which changed my momentary physiology? Did some memories arise in me, and if so, what did I do with them? Did I answer the questions correctly, and if not, what did I try to hide?
Definitions: What does “LGBTIQ*” mean? or “The 4 Dimensions of Sex”?
A lot of terms circulate around the issues of sex. A lot of people think they know what they are about. But sometimes it becomes clear that they do not know. The comment of the Mayor of Mannheim, Dr. Peter Kurz,2 “LGBTIQ? That’s too complicated! I welcome you by “hello all!” was not helpful. Levelling-out the differences between all these groups shows no interest in getting into the special situation of all the different groups of people and their special lives. Sometimes the term “non-heterosexuals” is used in the affirmative research of LGBTIQ* to make clear the suffering of all these groups as being devalued by the same heterocentrist society and culture, in which being a man with desires for women or being a woman with desires for men is the unquestioned base of a human sexual and loving being (Göth & Kohn, 2014). But the term, “non-heterosexuals” might not fit for trans* people who live in a heterosexual relationship after a sex reassignment surgery. Trans* people suffer instead from a world in which a cis3 identity is the unquestioned base of a human sexual and loving being. Hence, I would introduce here the term “non-cis-heteronormative” as a term, to sum up all LGBTIQ* in another term, knowing that this term is not perfect and could even be misunderstood.
Rather than this, the training team of PLUS tries to bring the diverse categories around the sexes in a comprehensive order by using the following 4 dimensions of sex, when they teach pupils or teachers, psychotherapists or social workers about the issues of LGBTIQ* people (Göth & Kohn, 2014):
| Biological Sex | Gender Identity |
| Sex Role | Sexual Orientation |
Dimension “Biological Sex” or What does intersex mean?
In this dimension we see the body, or analyze, it by (micro-)biology. It is the question about the physical aspects of being categorized as male or female: primary and secondary sex attributes, sex specific chromosomes, gonads, hormones. To simplify it: Look into the mirror and check what you see there: Do you see a man or a woman? Deviant from the hetero norms in this dimension are the terms intersexual, atypical sex attributes.
Some people are clearly categorized by their sex specific chromosomes but are irritated by some special deviancies in their body, like a man who experiences his breasts as too fat, more like female breasts; or a woman, who has a very traditional female figure, but some hairs sprouting between her female breasts. A lot of persons, who received the medical diagnosis “disorder of sex development”, feel devalued by this term. Since 2006 they have used the term “differences in sex development” and call themselves “inter*” or “intersex” (Günther, 2016). Inter*people who were adjusted by surgery directly after birth to the assumed sex, often suffer many medical and mental problems from this attempt to put the child into the binary system of female and male as soon as possible. Sometimes these problems start after the long period of latency in puberty, when the gender formation, sexual activities and orientation reach a new level.
Diversity of Sex
Western cultures are based on a dichotomy of sex. Before a baby is born, the most common question in ultrasound asked by the pregnant woman is: “Is my baby healthy?”; the second is: “Is it a boy or a girl?”. The clothing industry provides the color blue for boys and pink for girls from the very first days of life.
In contrast to this there is a third sex called “Hijra” as a government category in India and Pakistan, taking the Indian cultural tradition into account that there are more than male and female identities. Australia, New Zealand and Nepal try to get along with the new changes in society, allowing their inhabitants to choose a third category besides female and male. If the western dichotomy of sex would be skipped, intersexuality would no longer be a mistake of nature but a sign of its diversity. There would not be only two sexes among the nearly 7 billion number of human beings.
Dimension “Gender Identity” and “Trans…”
This dimension focuses sexuality on the psychological level or on the level of the core gender identity. This refers to the inner consciousness, sureness and confession of belonging to a particular sex. Here, the probably oversimplified question could be: Close your eyes, feel and experience what your gender could be: female or male? A lot of people who feel the same gender as they can face in the mirror are called “cisgender” or “cis” for short.
People, who experience a difference between the sex they were assumed at birth (similar to the biological sex of section 2.a) and their felt psychological sex, describe themselves with a wide range of self-designations. For some, the gap between the sex assumed at birth and the felt gender is so big, that they feel the urge to have gender transitioning by hormone replacement therapy. Or, if they are before or still at the puberty stage – at least, to seek a therapy that blocks the production of sexual hormones. After starting this therapy, they might have a sex reassignment surgery as a further step in gender transitioning. In this case some use the older term “transsexual” more frequently. Others, who do not feel so much defined by the “sexual” aspect but experience the gap more as a part of their personality, use the terms “transident” or “transgender”, “transwoman” or “transman”. And yet, others do not see the solution to keep on being stuck to one of the both categories of male or female and design themselves as “non-binary”. A term in which the most of those persons could feel themselves grouped together is “trans*” (Günther, 2016).
Dimension “Sex Role Identity”
This dimension is also called Social Sex and includes all behavior and experiences, personality attributes and functions, which social-culturally are typically referred to one sex. The simplified question here would be: What do you try to make the other think about your gender? Or: What is seen as male or female in your society?
Somebody who likes to present him- or herself in a transvested outfit, is found in this dimension.
Deviant from the hetero norm are terms like “sex-role-non-conform” or “atypical”, “androgyne”, “metrosexual”. Aspects of a sex role can be behavioral or attributes of a personality. Traditional definitions of men and women can be summarized as “not to be of the other sex”, “to have sex with the other gender”, “to concept children” or “bring children to earth”, “to finance a family” or “to raise children” (Heinrich & Reipen, 2003). In modern psychological research masculinity is found to be correlated with “instrumentality” (task and solution orientation: active, competitive, easy in decision taking); feminity is correlated with “expressivity” (able to get into contact with, friendly, warmly in relationship with others). Following this research, 4 types of people can be found: “feminine”, “masculine”, “androgen” (being feminine and masculine; 51.9% men; 48.1% women) and who are correlated with higher mental health, and fourthly, “indifferent” (being less feminine and masculine; 76,6% men; 23,4% women) (Altstötter-Gleich, 2000).
Dimension “Sexual Orientation” vs. Sexual Identity and Being a Star: Queer*
This dimension is the only one which is not about one’s own sex or gender, but about the gender of the sexual partner; hence, it is also called “sex partners orientation”. “Sexual Orientation” means the orientation of sexual and emotional needs of a human being towards human beings of the same sex, the opposite sex or towards both sexes. Thereby, an orientation onto the opposite sex is called heterosexual, onto the same sex is called homosexual, and onto both sexes is called bisexual” (Göth & Kohn, 2014, p. 6). Göth and Kohn distinguish between sexual behavior, desire, fantasies, orientation, and identity:
“Sexual Identity” defines the identity, which a person develops from his or her sexual orientation. This development is influenced by the individual, social and cultural situation, in which he or she is placed and lives in, and intersectionally influenced by further aspects of his or her identity.” (Göth & Kohn, 2014, p. 6). This might help to male clear, that a person who lives in a heterosexual marriage has kids and understands/identifies him or herself as heterosexual can have sexual contact with a person of the same sex. While sexual behavior occurs in all societies of today, the sexual identity of a lesbian woman or a gay man are only found in the so-called Western cultures.
The self-designation of the sexual identity is very wide in its range, starting from homosexual, gay, lesbian, women loving, bisexual, open minded to queer. Some people do not see themselves as well described in having a sexual identity at all. Other deviant terms from the hetero norm here are “homo- and bisexual”, “asexual”, “pansexual”, and “queer”. The terms of homo, hetero- and bisexual, are still in the grip of the dichotomy of sex in male and female. Furthermore, they are a trial to simplify the diversity of living by setting these categories.
Because there are so many terms for every dimension of sex, which people use to name themselves, it became usual to set a star at the end of the end of trans*, inter*, queer* and on the whole list of letters LGBTIQ* to welcome and include everybody who feels in one of these directions but uses another term for self-designation.
Statistics
As there is a great difference between the sexual orientation and the sexual identity as well as between sexual behavior and self-designation, numbers about the distribution of people who live homosexual differ a lot. Big random samples like the National Intimate Partner and Sexual Violence Survey (Walters et al., 2013) found that the sample of n = 9086 women designed themselves 1.3% as lesbian, 2.2% as bisexual. 2% of n = 7421 men designed themselves as gay, 1.2% as bisexual. Mercer et al. (2013) cited that 8% of the men interviewed had sexual contact with another man, 11.5% of the women had sexual contact with another woman. The numbers of the women increased to 18.5%, if they were between 16 and 34 years old.
Fluidity
Furthermore, results of more recent research show that the self-designation of sexual identity varies considerably over time. Diamond (2008) found out that more than two-thirds of women who were interviewed in a long-term study changed the self-description of their sexual identity at least once within 20 years – in both directions.
Sexual preference
A similar but different term to sexual orientation is sexual preference referring to the developmental state of the sexual partner from child to elderly. In many countries the laws against non-heterosexuals are based on pedosexual behavior. But research shows the difference of these two terms: quoting Göth and Kohn again, Beier et al. (2005) found out that pedophilia occurs almost exclusively in men of which 1% can be described with this term. Göth and Kohn quote the Gesundheitsberichterstattung des Bundes (Federal Health Report) that in 2012 girls have become victims of pedosexual violence a lot of times more than boys. These results make clear, that sexual orientation is not connected with sexual preference at all, which leads to sexual abuse, if practiced with children.
Do not categorize! Differentiate!
The four dimensions of sex are not for fixing human beings. In fact, a lesbian might find out that he is a trans*man and hetero. Gay guys might play with sex roles. And there might be a trans* person with an inter aspect living homosexual (Günther, 2016).
Special Aspects of LGBTIQ* Lives
As a gay man my experience and knowledge come first of all from the world of gay men. Some of the following concepts are also coming from a more homosexual perspective. Nevertheless, my colleagues at PLUS and I found some of them helpful for the work with trans* and intersexual* clients as well.
Internalized Homo-, Bi- and Trans-negativity
Living in a heterocentric world, we may get into contact with the categories of our social world earlier than with our own specific needs or being. To be a girl or a boy becomes important from an early age and is pretty clear around age 4. But even till then we have heard our family members and neighbors talking about the differences between male and female a thousand times. When puberty begins hormones start to flow and the body changes. Sexual arousal becomes more important than before. But until that time children have heard many times about “faggots” and “queers”. In German, the word for gay is “schwul (pronounciation: shvu:l)”, which is for these kids the complete opposite to “cool”, which is an expression of highest value for them.
So, we all have an idea about what a boy or girl is like and how valuable it is to be a homosexual or heterosexual, before we become conscious about the fact that these categories have something to do with our own life. Attitudes are often passed by our social models from one generation to the other which are mostly shaped by the paternal figures, peers, and more and more by the contents of mass media and social media. At least at the beginning of our life we do not experience the content of these attitudes as much. In this way they are not grounded in experience, but they are more likely prejudices.
Because they refer to basic categories of our human understanding, they are very important. Hence, they are giving us an orientation about what is worthy and less worthy (like women are still less worthy than men even in the Western culture, which is seen by the structural discrimination that women earn less money for the same jobs). Finally, these cis-heteronormative concepts of sex, gender and sexual orientation are internalized more or less by all members of a society. But if someone is part of the non-heterosexual-cis society, these concepts do not give only a frame for one’s own point of view on the outer world but are attached to one’s own person. This internalized homo-, bi- or trans-negativity hinders a LGBTIQ* to take an easy path to self-esteem and self-security. More than that, these attitudes hinder a supportive contact with other persons of the same non-cis-heteronormative art of living and by this the possibility to empower oneself by sharing experiences with others who have a similar way of life.
Model of Non-Cis-Heteronormative Identities Formation
Vivian Cass (1979, 1996) showed in her model of homosexual identity formation a very helpful tool for the counseling and therapy of homosexual clients. According to my opinion the expansion of this model to all non-cis-heteronormative identities and their formations is helpful. Following Cass’ model, the beginning of the development of a LGBTIQ* person starts on a pre-step, in which the person experiences her- or himself as being part of the heterocentric society, so to speak as a heterosexual cis person does. Another important aspect of her model is that she divides the process into many different stages. These could be crossed over in a few big steps only, but it is possible as well to stay on one step for a longer period. A third important aspect is, that she does not devalue any solution of a stage, neither the solution of a person who accepts the new aspect of her or his life, nor the one who denies it and ends the process in a foreclosure.
The different stages (originally there were seven) can be grouped together into those which are describing the inner process of a coming-out of self-acceptance of the own gender or sexual identity and those of a coming-out process in which a person makes contact with others of the same and of other dimensions of sex. Finally, Cass’ model helps to find a language in which a therapist can talk to a person, who is at a special stage. It offers furthermore an understanding why partners in a gay or lesbian relationship or a relationship with two intersexual or trans*persons might have special problems to solve, if the partners are on different stages of their gender or sexual identity formation.
Coming-out
The most different experience of LGBTIQ* in comparison to cis-heterosexuals is that at a certain point in their lives they have to ask themselves, whether they differ from others regarding to their sex, gender or sexual orientation with all its implications, as described by Vivian Cass (1979).
But this is not only an inner or a cognitive process. It is always a holistic experience with oneself and in contact with the social world. Biechele found out that the most common emotional state of gay young men in Germany of 1999 were lovesickness (54% of the participants) and solitude (47%) besides some more special gay issues like the following: worrying about AIDS (39%) and “How can I get to know other gay guys?” (37%). Therefore, solitude is not only a strong emotional state in the pre-coming-out phase but is an ongoing issue at least during the time gay young men find their own place in the community. Researchers in Berlin found in 1999 that gay and lesbian teenagers are four times more suicidal than the heterosexual peers (Berlin, 1999). More than 25% of gay men experience that their fathers do not accept them after they know they call themselves gay (Biechele, 2009).
To fall in love and to have sex for the first time happens almost at the same age with lesbians, gays and heterosexuals: between 16.6 and 17.1 years (Biechele, 2009 and Berlin, 1999). Nevertheless, there are basic differences between these groups. The first sex partners in heterosexual couples differ only by 1.3 years of age. In contrast, the first sexual partner of gay men is on average 6 years older than themselves. He is 10 years older or even more in 14% of gay men. This means that the gay men’s “first time” is not embedded in peer sexual encounter, in which both might have the same or a similar level of experience (Biechele, 2009). On the other end, the first sex partners of lesbians are men in 66% of cases. That means their first sexual encounter is a heterosexual one (Berlin, 1999).
In the process of gender transitioning in Germany at present, trans*people are forced to live overtly in their everyday life as a necessary condition to get the hormone replacement therapy and the sex reassignment surgery. This builds up a big pressure and hinders a self-imposed development (Günther, 2016).
Experiences of Discrimination
All LGBTIQ* have experienced discrimination or even violence because they are LGBTIQ*. 100% of the participants in a study at PLUS e. V. of 2006 reported experiencing verbal discrimination at least once in their life because of their sexual orientation (Haas & Göth, 2006). This result allows me to assume that this applies to trans* and inter*sexual people as well. Of course, the manner and situations in which discrimination and violence take place differ a lot between the different groups of LGBTIQ* and they even differ in the subgroups according to the place/state where they live. Trans* and inter persons are more likely visible as different from the heterosexual norm. Gay men and lesbians are more likely visible if they are in public as a couple or together with friends. On the contrary, Bisexuals might stay invisible and have more likely to tell others about their sexual orientation to introduce themselves as bisexual.
In some countries, homosexuality is prosecuted to death by law, i. e. in Saudi-Arabia or Iran. On the other hand, Iran is one of the countries where sex reassignment surgeries are frequently done. Nevertheless, this is not an argument for an open and diverse society, but the possibility of adjusting inhabitants to the binary system of male and female, which supports the patriarchal system of the country.
Living in the Western hemisphere, it seems as if the laws for LGBTIQ* improved to a more liberal attitude during the last decades. This was affirmed again in July 2017, when the German parliament voted for equal heterosexual and homosexual marriages. But as the developments in Russia, Turkey and the USA have shown during the past few years, culminating in the decision of president Trump in August 2017 against trans*persons being in the army, that the development does not only go in one-direction. Furthermore, LGBTIQ* lives are always on display and are supposed to have a quick role back in a society. Hence, there is a great need for political commitment and psychotherapeutic support to maintain the liberties essential for diversity.
Even in countries where there is no prosecution according to sexual orientation or gender identity, LGBTIQ* suffer a lot from discrimination and violence. Two-thirds of the participants of the referred PLUS study experienced psychological violence. Physical violence hits gay men and lesbians almost the same in quantity (still 2%) but not in quality: physical violence against gay men was done more by foreigners in a non-sexual way and in public space; lesbians experienced more sexual physical violence by relatives or (ex-)husbands according to the coming-out process (Haas & Göth, 2006).
Günther (2016) indicates that people like trans* and inter* with a not distinctly male or female appearance become likely victims of discrimination and violence. She points out that the early medical surgeries to adjust inter*persons to the sex which was assumed by birth, is violence and could be compared with sexual violence and forced genital mutilation.
Minority Stress Model
Before affirmative research on non-heterosexual lives started, the research on LGBTIQ* took place in the offices of psychotherapists and hospitals. In the results of their research, LGBTIQ* were seen per se as ill. But even after the start of affirmative research there were still significant differences found in surveys about a special disease in the percentage of hetero and non-heterosexual clients. Ian Meyers (1995, 2003) did a meta-study of many of those surveys. He found significant results between heterosexuals and lesbians or heterosexuals and gay men or heterosexuals and bisexual women or men over different mental diseases in several studies. Furthermore, the group which was more severely ill was always one of the non-heterosexual clients. But he found no repetition of the significant results about a special disease over different studies. Ian Meyer concluded that these findings may be part of a minority stress, which is an additive stress to people who do not belong to the majority. Minority stress includes the larger effort to get into contact with the other members of the same minority, as well as to withstand the daily devaluation of discrimination.
It became clear as well that a non-heterosexual identity per se is not enough to provoke a difference in one single study. But if there is vulnerability in a person caused by the situation or individual aspects, the minority stress might be the drop which makes the barrel overflow. Meyer’s concept is built up on the population of LGB*, but his explanation supports the conclusion that the process of minority stress can be applied to TIQ* as well.
Intersectional Aspects
Another aspect can be isolated during the last years of research. Kimberlé Williams Crenshaw could outline that the most affected employees by a decision of job cancellation at GM in the 1980 were not Afro-American men or White American Women but Afro-American women (Crenshaw, 1989). People affected by a double- or multi-discrimination as women of color or lesbians (= women and homosexual) or transsexual gay men (= transsexual and homosexual) suffer stronger in terms of mental health issues than people suffering from one kind of discrimination only.
Shaping of Relationships
Acknowledging in the last sections that there are special aspects in a LGBTIQ* life and that the aspects between the different groups of non-cis-heteronormative persons differ as well, it could be supposed that to build a relationship might have special problems for LGBTIQ* on top of the usual difficulties in a heterosexual cis relationship. This surplus of problems together with the frequent lack of children as a stabilizing triangulating factor makes it more difficult for LGBTIQ* to live in a stable relationship. Nevertheless, Michael Bochow can show that during the last 30 years since 1987 approximately 50% of gay men are in relationships, the majority of which last longer than 10 years (Bochow, 1989; Bochow, Schmidt & Grote, 2010).
The counselor team of PLUS found out that there are great differences in the issues that gay and lesbian couples have to deal with. Ulli Biechele and I experienced that our gay couples are often coming into couple counseling in a very late stage of a relationship crisis when it is almost impossible to find a constructive solution. Another solution we found is that only one partner tries to solve the couple’s problems in a single counseling, because the other partner is not willing to join. Our lesbian colleagues Margret Göth and Andrea Lang sometimes do not start couple counseling or end it up early, when they find out that a couple’s problems are not couple specific, but that they are confronted with a complex of problems with which each partner has to deal separately within single therapy.
Besides these more gender specific dynamics there are some special issues, with which gay or lesbian couples have to deal with, which does not occur in heterosexual couples: differences of coming out status or different experiences with anti-homosexual violence up to hate crimes (see section 3.e).
On top of these, there are some issues, which could occur in heterosexual cis couples as well, but are less common there, e. g. discordant HIV-status, which concerns gay couples especially. Secondly, there is also a difference in culture. Here the couple’s dynamics of being exotic for each other is not the only important aspect, but there are also the different experiences of having been discriminated, i. e. by laws towards their own LGBTIQ* life in the different home countries and towards the foreign partner in the country of the other. Thirdly, there is a difference in social and economic status. Because of the minority status and the change of community and social network during coming out, there is a higher degree of need to be open to find a partner on a different social level or with a different social and economic status in LGBTIQ*. Fourthly, there are also more long-distance relationships. Because travelling has an important impact on meeting possible partners as members of minorities, those partnerships are more likely to be long-distance relationships. There is, fifthly, the concept of open relationships in contrast to sexual fidelity. Because the traditional relationship patterns assume a relationship based on sexual fidelity between a man and a woman, it might be more frequent for gay men and lesbians to negotiate a concept which fits better to them. Bochow (1989; Bochow, Schmidt & Grote, 2010) found in his surveys that approximately 50% of the participating gay men define their relationships as open and the other 50% as monogamous. Heterosexual couples have started to do this as well more and more, but still are less open and very much more defined as monogamous. Sixthly, there are problems with a conception of a child by genital sex. Over the last 20 years the wish of lesbians and gay men to become mothers and fathers has increased steadily. Some gay men and lesbians already had children in an earlier heterosexual life (gay fathers and lesbian mothers). Others choose non-same-sex persons, with whom they can plan and bring a child into the world for a so-called “rainbow family”. Different patterns of responsibility for the children have to be negotiated between the biological parents and their social co-mothers and fathers. On the way of a trans* identity formation there is a step, where the person has to think of taking an egg cell or sperm sample to freeze to preserve the possibility of having children later, before starting hormone replacement therapy or sex reassignment surgery.
Counseling and Therapy with Relatives of LGBTIQ*
As we could see in section 2.d.1 the proportion of LGB* in the population is quite small, and so are the statistics of TIQ* as well. Counting all big recent sample surveys together the sum of LGBTIQ* is between 8% and 25% of the population depending on how the surveys are structured in their questionnaires (sexual orientation vs. sexual identity, transsexual vs. transgender, etc.). But because of the impact of a coming-out as a LGBTIQ* person on his or her family and back onto the LGBTIQ* person in form of discrimination or even violence, relatives frequently develop pretty a great need for counseling and sometimes even therapy as well (Günther, 2016).
Adoption of the Point of View of LGBTIQ*: Clouds of Thoughts
An example for a method to help the participants to change their point of view into a LGT* child is Ralph Kohn’s “Clouds of Thoughts”. It was further developed at the workshops of PLUS about LGBTIQ* lives, and is used nowadays in the following form:
At first, the participants of the workshop are asked to write down expressions they heard in former times, which described “gay guys”, “lesbians” and “trans*people”, putting each expression on a card. The expressions about gay guys are put on a pink card, those about lesbians on a blue card, and those about trans* on a white card. During a short break, the trainers sort and pin the cards of each color on a flipchart paper around a drawn head. Then the participants are informed that they will be told 3 stories about three different children. Before that, all of them are asked to find a comfortable position and close their eyes, if they want. In what follows, they can accompany each child and get a feeling or an image how the child will feel and what they will do next. One of the trainers tells a short story about an 11-year-old boy, who had his first nocturnal pollution and feels strangely excited. When he meets his class mate, the boy asks himself, “could it be that I am gay? – but a gay guy is …” And afterwards, every card is read aloud. If some cards have the same expression written on it, this expression will be read as often as it was written, which enhances the expression. After the end of the story the participants are asked, “How does that boy feel? What will he do next?” The following discussion brings the empathic answers of the participants together. After this, the second story about an 11-year-old girl who asks herself if she could be lesbian, is told and discussed. Finally, the third story is told about an 8-year-old child, who does not feel comfortable with his or her gender, which is said to belong to him or her since birth. At the end, all three experiences of the participants are compared and discussed.
Courses of Action: Considerations for an Affirmative Bioenergetic Therapy with LGBTIQ*
Being aware of these differences in social, emotional and body related lives between cis heterosexuals and LGBTIQ* as well as between the LGBTIQ* subgroups, it might become clear, that a Bioenergetic therapist has to deal with different issues in the work with LGBTIQ* clients than in the work with heterosexuals. Summarizing the differences listed above, a Bioenergetic therapist should expect that his or her LGBTIQ* client has already dealt with confusion, loneliness, minority experiences, devaluation, discrimination, violence and hate with all the consequences on an emotional level like depression, anxiety, self-hate, PTSD, and even deep personality disorders. How can Bioenergetic therapists prepare themselves for their work with clients traumatized in this specific way?
As the training project POWER UP of PLUS could identify in its evaluation (Lang, Reipen & Heinrich, 2007) a set of proven courses of action helped to change attitudes towards LGBTIQ*. Following this, it might be important for a work with LGBTIQ* clients to get a clear orientation, how to do deal with the large amount of information and the newly found point of empathic view on these potential groups.
Günther (2016) points out the importance of considering that real bodily potentials are made invisible or are destroyed in inter* persons; therefore, the issues of those clients might be oriented at first more towards the loss of physicality than towards the future. Trans* persons often suffer from a specific body related hostility, she calls “Bodyism”, because the body would not suit the cis-body norm. This hostility would be mostly combined with sexism. These short statements may help a therapist to realize on which level body work with LGBTIQ* clients is needed.
Stein and Burg (1996) listed “Educational objectives for a gay affirmative training”. Margret Göth and I (Heinrich & Reipen, 2001) developed further considerations for the training for psychotherapists of gay, lesbian and bisexual clients. Mari Günther (2016) created guidelines for counselors of trans* and inter clients. Based on these lists I built up a very short guideline for the work of Bioenergetic Therapists with LGBTIQ* clients:
- Knowledge about the listed issues above (sections 2, 3 above), plus knowing the history of the development of aspects of laws, scientific theories and affirmative research concerning LGBTIQ* helps to get an idea of what LGBTIQ* clients may already have experienced. It might help to see your LGBTIQ*client as a worthy human being in its special life situation and not a client suffering from a specific defect. Furthermore, it might help to find a language to talk to them about their stage of sexual orientation and their gender identity, about their loves and lives.
- Knowledge about the LGBTIQ* community helps to support LGBTIQ* clients to find contact to peer or support groups in reality and to use the internet to support a LGBTIQ* self-affirmative and determined life.
- Knowledge about the oedipal triad which profoundly differs in LGBTIQ* clients (Isay, 1989, Giesrau, 1993) helps to find early experiences of being rejected by primary caretakers.
- Reflecting one’s own experience as a member of a minority, if applicable, and the discrimination which derives from it, helps empathize with LGBTIQ* clients.
- Reflecting one’s own somatic resonance, transference and countertransference and its specific parts to the issue of LGBTIQ* helps to become aware of the traps of an underlying LGBTIQ* negativity and the limits of one’s own empathy
- Being aware of these limits of empathy towards the client helps to find an authentic contact and relationship with the client, where further development can take place.
This list might discourage feeling able to become a good Bioenergetic therapist for LGBTIQ*, if someone has no contact to this world by one’s own sexual orientation or gender identity, relatives or friends. 0n the other hand, not every LGBTIQ* Bioenergetic therapist is a good therapist for LGBTIQ* clients per se. It needs the joy and curiosity to step into this world of diversity and to reflect the own reactions in this cosmos. If information about the world of LGBTIQ* and their communities is not on display, supervisors or colleagues might know where to get them, or an internet research might help. Asking LGBTIQ* clients for information would be a misuse of the client.
In the end, LGBTIQ* clients are worthy to have the choice of selecting a good Bioenergetic therapist for themselves, someone who fits them and their stage of identity formation – some need LGBTIQ* therapists, some need hetero cis therapists.
PLUS Bioenergetic Workshops
To provide a more practical view on this field how this could be implemented, I will end with a short account of my work with LGBTIQ* over the past few years. PLUS has offered a semiannual Bioenergetic workshop series for gay and bisexual men for the past 14 years. These workshops start on Friday evening and end on Sunday early afternoon. They include classical Bioenergetic exercises and working in dyads and body contact with the whole group. After each body-oriented series of exercises a round of sharing experiences takes place, where the participants also give comments about how they are touched by the feedback of another man. Over the last few years, one of the workshops was client orientated, the other had a theme like “Body language and self-expression” or “Untouchable”, where a certain issue close to a gay man’s life was the focus of the weekend.
In the last workshop in May 2017, I asked the 8 participants about the benefits they got from these workshops. Every gay or bisexual man of this group had participated in the Bioenergetic workshops 2 to 10 times. The most used word as an answer was “selbstverständlich”, which could be translated by “naturally”, “as a matter of course” or “self-evident”. This word was connected with “non-sexual body contact with other men”, and a “not conformist contact with other gay men”. The last phrase is also set in contrast to the gay community, which is often referred as cold, superficial, categorizing. The participants report that they came into contact with their needs as gay men by the Bioenergetic work in the group. They found ways to live a self-determined gay life independently from their own categories about how they have to live as a gay or bisexual man, which derived from the heterocentrist world as well as from the gay community they were living in.
In single counseling with gay men and lesbians at PLUS, the main issues are mental health, coming-out, contact to other gay men and lesbians individually as well as with the community, difficulties in or with partnership, violence and internalized homo-negativity. The work with internalized homo-negativity, (as well as about trans-negativity and inter-negativity) needs knowledge about the first time LGBTIQ* clients received information about their own specific LGBTIQ* subgroup. This information was often given by parents, the media or in school (and as I mentioned, “schwul” (gay) is the most frequent swearword at German schools). LGBTIQ* clients often experienced a lot of violence and mobbing, devaluation and hate in that time of their lives, because of their not being part of the heterosexual cis majority. This traumatization can cause an introjection of the perpetrator to stabilize oneself. The work with this ego-state needs a lot of emotional grounding and empathetic standing for the Bioenergetic therapist.
In my Bioenergetic practice I frequently work with body contact to bring gay men into their strength and power. This is easier in a workshop, because the clients can see that their experience is not only their personal one, but one almost all of them share.
A special development has taken place at PLUS over the past 5 years. More and more trans*people have come and asked for help. In 2016 there were so many trans*teenager clients, that we decided to establish a youth group for trans*teenager from age 13 to 22 years. The CO team of PLUS gave me as a mostly cis gay man the task of being part of the leading team at the beginning to bring the culture of PLUS to the leading team and the group. Searching for co-leaders in October 2016 I had found two in November. At the first meeting in January 2017, 5 teenagers participated. Every week there is a new one asking for counseling in the Centre and has been coming to the group. On average, there are 5 teenagers at each meeting, some come very regularly, some are more circling around the group. I could not start with Bioenergetic work yet with this group. But it is clearly perceptible, how the teenagers flourish on a physiological and behavioral level by being given the frame of being accepted as they are in their own variety of sex, and by finally finding others where they feel at home and understood.
References
Altstötter-Gleich, Chr. (2000). Möglichkeiten der Operationalisierung von Expressivität und Instrumentalität. Entwicklung von Skalen zur Erfassung der Geschlechtstypizität (GTS). Forschungsberichte des Fachbereichs 8. Psychologie, 23, Universität Koblenz-Landau, Abteilung Landau.
Baum, S. (2008). Fathers are the Dark Matter of the Psychic Universe. Bioenergetic Analysis, 18: 93–109. Gießen: Psychosozial.
Beier, K. M., Bosinski, H. A. G. & Loewitt, K. K. (2005). Sexualmedizin. Grundlagen und Praxis. 2nd ed. München: Elsevier, Urban & Fischer.
Biechele, U. (2009). Identitätsentwicklung schwuler Jugendlicher. Saarbrücken: Südwestdeutscher Verlag für Hochschulschriften.
Biechele, U., Hammelstein, Ph. & Heinrich, Th. (2006). Anders verrückt?! Lesben und Schwule in der Psychiatrie. Jahrbuch Lesben – Schwule – Psychologie 2006. Lengerich: Pabst Science Publishers.
Bochow, M. (1989). AIDS. Wie leben schwule Männer heute? Bericht über eine Befragung im Auftrag der Deutschen AIDS-Hilfe. 2nd ed. 1989. Berlin: Deutsche AIDS-Hilfe e. V., 123 pp.
Bochow, M., Schmidt, A. J. & Grote, S. (2010). Schwule Männer und HIV/AIDS: Lebensstile, Szene, Sex 2007. Berlin: AIDS-Forum DAH. Bd. 55.
Cass, V. M. (1979). Homosexual identity formation: A theoretical model. Journal of Homosexuality, 4: 219–235.
Cass, V. M. (1996). Sexual orientation identity formation: A Western phenomenon. In Cabaj, R. P. & Stein, T. S., Textbook of Homosexuality and Mental Health. Washington: American Psychiatrie Press, 227–251.
Cockburn, G. (2008). Standing on both legs: A Bioenergetic Perspective on the Family, Gender Roles and the Development of the Self in the 21st Century. Bioenergetic Analysis 18: 11–26. Gießen: Psychosozial.
Crenshaw, K. (1989). Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine. The University of Chicago Legal Forum, Vol. 1989: 139–167.
Diamond, L. M. (2008). Sexual fluidity. Cambridge: Harvard University Press.
Gissrau, B. (1993). Die Sehnsucht der Frau nach der Frau. Psychoanalyse und weibliche Homosexualität. Hamburg: dtv.
Göth, M. & Kohn, R. (2014). Sexuelle Orientierung in Psychotherapie und Beratung. Berlin Heidelberg: Springer.
Günther, M. (2016). Psychosoziale Beratung von inter* und trans* Personen und ihren Angehörigen. Ein Leitfaden. Frankfurt: pro familia Bundesverband. https://www.profamilia.de/fileadmin/publikationen/Fachpublikationen/Inter_Trans_Beratung_Leitfaden.pdf
Haas, B. & Göth, M. (2006). “Schwule klatschen und Mannweiber anpöbeln” – Onlinebefragung zu Gewalt- und Diskriminierungserfahrungen bei Lesben und Schwulen in der Rhein-Neckar-Region. Mannheim: PLUS e. V. http://www.plus-mannheim.de/images/stories/gewaltstudie.pdf
Heinrich, Th. (2015). Workshop 2: Begleitung nicht-heterosexueller Jugendlichen. Workshopbericht. In PLUS e. V. (Ed.), “lesbisch, schwul und noch viel mehr” Fachtagung zu intersektionalen Ansätzen in der Praxis 05.Oktober 2015, Hochschule Mannheim. 32. Edenkoben: Flyerdienst Weber UG. http://www.plus-mannheim.de/images/stories/Doku_LesbischSchwulVielmehr.pdf
Heinrich, Th. & Biechele, U. (2006). Das Mannheimer RISPE-Projekt. In: Hammelstein, Ph, Biecele, U. & Heinrich, Th., Anders verrückt?! Lesben und Schwule in der Psychiatrie. Jahrbuch Lesben – Schwule – Psychologie 2006. Lengerich: Pabst Science Publishers.
Heinrich, Th. & Reipen, M. (2001). Gay Men and Lesbians – Clients of Unknown Species. In Steffens, M. C. & Biechele, U. (eds.), Review of Lesbian, Gay, and Bisexual Issues in European Psychology. Trier: ALGBP, 125–141.
Heinrich, Th. & Reipen, M. (2003). Weiblichkeit und Männlichkeit in der Lesben- und Schwuleneratung. In Steffens, M. C. & Ise, M. (Ed.) Jahrbuch Lesben- Schwule – Psychologie. Lengerich: Pabst.
Heinrich, Th. & Kohn, R. (2006). “Jetzt hab ich verstanden, worum es Euch geht!” Erfahrungen aus der Aufklärungsarbeit von PLUS e. V. zur Homosexualität in Klassen und Jugendgruppen. In PLUS. Psychologische Lesben- und Schwulenberatung Rhein-Neckar e. V. (Ed.), Also, wenn Bienchen mit Bienchen … Von der bunten Vielfalt der ersten Liebe. Fachtagung vom 12.12.2005 in Mannheim. Mannheim: PLUS. http://www.plus-mannheim.de/images/stories/FachtagungPOWER-UP.pdf
Hooker, E. (1957). The adjustment of the male overt homosexual. Journal of Projective Techniques, 21: 18–31.
Isay, R. (1989). Being homosexual. Gay men and their development. New York: Farrar, Straus, and Giroux.
Klein, F. (1993). The Bisexual Option. 2nd ed. New York: Haworth Press.
Klein, F., Sepekoff, B. & Wolf, T. J. (1985). Sexual Orientation: A multivariante dynamic process. J of Homosexuality, 11: 35–49.
Lang, A., Reipen, M. & Heinrich, Th. (2007). “Das sind ganz normale Menschen auch”. Evaluation des Projektes POWER UP – Förderung eines angemessenen professionellen Umgangs mit Jugendlichen auf der Suche nach ihrer sexuellen Identität in verschiedenen Bereichen der Jugendhilfe. Mannheim: PLUS e. V.
Lowen, A. (1965). Love and Orgasm. New York: Macmillan Publishing Co.
Mercer, C. H., Tanton, C., Prah, P., Erens, B., Sonnenberg, P., Clifton, S., Macdowall, W., Lewis, R., Field, N., Datta, J., Copas, A. J., Phelps, A., Wellings K. & Johnson, A. M. (2013). Changes in sexual attitudes and lifestyles in Britain through the life course and over time: findings from the National Survey of Sexual Attitudes and Lifestyles (Natsal). The Lancet, 382 (9907): 1781–1794.
Meyer, I. M. (1995). Minority Stress and Mental Health in Gay Men. Journal of Health and Social Behavior, 36(1): 38–56.
Meyer, I. M. (2003). Prejudice, Social Stress and Mental Health in Lesbian, Gay and Bisexual Populations: Conceptual Issues and Research Evidence. Psychological Bulletin, 129(5): 674–697.
Rado, S. (1940). A Critical Examination of the Concept of Bisexuality. Psy Som Med, 2: 459–467.
Senatsverwaltung für Schule, Jugend und Sport, Fachbereich gleichgeschlechtliche Lebensweisen (Ed.) (1999). Sie liebt sie. Er liebt ihn. Eine Studie zur Psychosozialen Situation junger Lesben, Schwuler und Bisexueller in Berlin.
Socarides, C. (1968). The Overt Homosexual. New York: Grune & Stratton.
Walters, M. L., Chen, J. & Breiding, M. J. (2013). The National Intimate Partner and Sexual Violence Survey (NISVS): 2010 Findings on Victimization by Sexual Orientation. National Center for Injury Prevention and Control. Atlanta: Centers for Disease Control and Prevention.
About the Author
Thomas Heinrich, Dipl.-Psych., Certified Advanced RolferTM, CBT since 2001, member of the Süddeutsche Gesellschaft für Bioenergetische Analyse (SGfBA) and member of faculty of the IIBA, has focused in the last years on the anatomical basics of Bioenergetic Analysis especially in the work with traumatized clients and those with non-heterosexual orientation and transgender. Private practice in Mannheim, Southern Germany. Founder and counselor at PLUS. Psychologische Lesben- und Schwulenberatung Rhein-Neckar (Psychological Lesbian and Gay Councelling Center), Mannheim.
info@praxis-thomas-heinrich.de
Endnotes
- [1]
- My thanks go to my colleagues of PLUS, especially Margret Göth and Ulli Biechele, with whom I built up and led the counseling center in Mannheim for over 17 years, and to Angelika Wenzel, who polished this article in understandable English.
- [2]
- At the Beteiligungsworkshops zum Aktionsplan “Für Akzeptanz und gleiche Rechte Baden-Württemberg”, a Conference of the Ministry of Social Affairs of the Region Baden-Württemberg, held in Mannheim, February 8th, 2014.
- [3]
- Cisgender: the gender identity aligns with the gender the person was assigned at birth.