Uses of the Sphere as a Motherfied Object in Bioenergetic Analysis
Julia Cegatti and Leticia Polosecki
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2018 (28), 99-118
https://doi.org/10.30820/0743-4804-2018-28-99 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstract: In this article we are going to present a “Biospheres” practice. It evolved as a result of integrating our formative experiences in Bioenergetics Analysis with the “Dynamic Sphere Postural Reorganization” (Esferodinamia Reorganización Postural, which will be referred to as “RP” technique). We describe the sphere (large rubber ball) qualities and how it can be helpful for body psychotherapy interventions. Finally, we look into two cases using this clinical tool. The sphere becomes an element that facilitates clinical and educational work in the contemporary Bioenergetic field.
Key words: Biospheres, Esferodinamia Reorganizacion Postural, RP, bioenergetics
Introduction
In 2010 we created Biospheres, a specific practice and exploration path that brings together and links our formative and work experience as Bioenergetic Analysts and as Esferodinamia Reorganización Postural (RP)1 instructors.
In this article we intend to conceptualize our findings and consider how they integrate and appear in our clinical and teaching activities.
Some questions that guided our reflection were: How do we use spheres to increase the multiple nuances of our inner sensations? How do their characteristics accompany us in the construction of a Bioenergetic experience? How do they contribute to clinical work and training? Which qualities do clients find with spheres that enable them to construct a somatic experience?
To deepen these inquiries we will systematize sphere qualities and present clinical examples of how it can be a contribution for the psycho-corporal therapist and teacher in the contemporary Bioenergetic field.
Brief Outline of RP
Esferodinamia Reorganización Postural (RP) is a technique created in Argentina by Alma Falkenberg2 in the eighties, based on Swiss experiences in which spheres were used to treat neurological disorders and on American experiences in which they were used to study movement patterns. In Argentina, thanks to research carried out by Alma Falkenberg’s disciples (such as Anabella Lozano), this technique is still being developed, with an ever increasing amount of outreach (Lozano, Cegatti, Martínez, 2012). During our training process as RP instructors we initially discovered that many Somatic Education3 and Bioenergetic principles are aligned.
Biospheres
In order to clearly define the specific practice that arises from this interaction, we shall refer to the work as “Biospheres.” In this section, we will characterize our main focus, basing our ideas on the theory of Bioenergetic Analysis posited by Reich and later adopted by Lowen, as well as some aspects of the principles governing RP.
The core ideas are:
- Body and mind are a unit.
- All psychological processes have a correlated physical process.
- Breathing is essential for the production of body energy and its restriction helps repress unbearable emotions.
- The importance of working with muscle tone: a) working on chronic muscle blocks and helping to ease tension, understanding their origins and function, and letting out the emotions they hold back and b) exploring different muscle tones and opportunities for self-regulation through dialog with the environment. Through the sphere we can shift our relationship with gravity, making it easier to change our muscle tone, its relationship with our weight and our tension levels.
- The concept of “grounding” as contact with our internal and external realities.
- Increasing proprioceptive realizations by means of the ball, mainly due to its chances of increasing “haptic” (linking touch to other senses) sensitivity.
Both RP and Bioenergetic therapy require the construction of a relationship where the original (developmental wound) sequence is not repeated, that is: frustration, energetic withdrawal and adaptive response. Current Bioenergetics also includes the principle of bonding. In the last 35 years, some colleagues at the International Institute (Robert Hilton, Robert Lewis and Guy Tonella, among others) have integrated developments on primary bonding and object relations into Bioenergetic Analysis, thus providing us with tools for addressing the growing difficulties of clinical work in psychology. According to Bioenergetic therapist Ana Krsul (Krsul, 2013), “An essential tool in this outlook is the therapist-patient bond as a path toward resilient transformation.”
Therapy is a co-creation of both patient and therapist, which integrates the dimensions of body, emotions, analysis, and bonds. The aim is to provide relief and induce the enjoyment of pleasure, joy, love and vibrant health, which were all blocked in the course of our history, bringing about changes in the body and the mind. These considerations do not account for all the complexities of the therapy nor, therefore, of the therapist-patient relationship. However, in this paper we are primarily interested in contextualizing our understanding of the importance of the sphere as a valuable tool for clinical work.
In order to show the multidimensionality of this tool, we systematize some characteristics of the sphere that we have discovered in our practice.
The Sphere: a Motherified Object
Filling up the Sphere with Senses
Different sphere uses create different perceptions and proprioceptive realizations. Knowing how to use the sphere provides the trainer or therapist with a toolkit for client support on the path toward recovering vital energy. Exploring the sphere enriches the client’s construction of his somatic experiences. By virtue of being an excellent object, it facilitates trust-based bonding, the bedrock for a therapeutic connection inspiring confidence that may result in a healing process. Its qualities further allow the therapist to read the client’s body and to work on issues such as contact, tenderness, aggression, assertiveness and congruence with sexuality, the latter being an area of expression of the client’s vitality. Work with the sphere creates an easy way to listen to how the patient tells their story, revealing defenses, struggles, affects and energetic movements such as contraction, expansion, flow or lack of flow. Because it includes the therapist’s body, it allows for therapeutic experiences in which qualities of the intersubjective relationship4 become apparent: the therapist resonates with the patient as their defenses rupture and old wounds are healed. In terms of contemporary Bioenergetics, this implies a real somatic and relational process (Fauser, 2015).
The aim of the classification that follows is to clarify our conceptual framework. Be it noted that in practice all of these functions occur simultaneously. Moreover, the practices sketched below are but a sample out of a wide array of possible choices.
Some of the qualities we have found are:
Increases perceptive and proprioceptive realizations: The sphere’s plasticity increases internal resonance of that which inhabits the body, facilitating its access to conscience. To quote one our clients, “it lets us be touched and it would seem to let itself be touched.” It is permeable to the client’s contributions and it makes contact back.
Transitional: We use the sphere as a motherified object insofar as it provides us with safety and tenderness. It fixes early experiences in which the primary attachment bond failed to provide safety. We observe that some clients may take it as a transitional object, insofar as it is a gateway into other practices. During child development, toys are transitional objects as they mitigate absences from a very early age. Some clients fetch the ball or ask for it as soon as they enter the therapist’s office. They allow themselves to express their tenderness toward the ball through the construction of a bond that creates some degree of freedom to ask for it and “possess” it. Some have gone so far as to name the ball. There remains the question of whether the sphere is in this sense a transition toward the therapist, which later expands into other forms of bonding.
Playful: In our culture a ball is a toy that is preserved up until adulthood through sport or leisure activities. This charge that characterizes the “ball” as an object causes it to be perceived as a friendly object, easily recalling the client’s playfulness and helping them to rediscover the joy of playing and living which, in Lowen’s opinion (Lowen, 1997), adults rarely experience. In this sense, we underscore what authors such as Freud (1988) and Winnicott (1972) reveal by construing games as a key element in infant growth and as an item of treatment and healing in the process of self-inquiry.
Facilitates erogenization: It allows for erogenization, i. e. it activates the skin’s sensory perception without running the risk of hypererotization. This function is of paramount importance insofar as it gives both the child and the adult receiving therapy the possibility to undergo sensations of pleasure that provide a foundation for the construction of their psycho-corporal continuity, a task that begins at birth, during the sensory-oral attachment phase (Tonella, 2013).
Containing: Contact with the sphere becomes a membrane regulating exchanges between the inside and the outside. It collaborates in the construction of an experience of a fitted attachment bond, which contains but does not retain. In this sense, we observe that after experiencing work with the sphere, several of our clients decide to purchase it and take it home as a resource for daily contact and self-regulation.
Holding: It is a facilitating element for those who need to re-experience holding, be it due to a lack of it, a distortion or an excess. It is an object that allows us to connect, something vital in the process of re-editing a primary experience of holding, without the commitment of doing it with another person’s skin. Letting out weight onto the sphere, which is necessary for it to remain stable, is thus an invitation to gradually release muscle tension. As a result, energy previously stored in myofascial fibers becomes available as vital energy. For some of our clients, letting out weight onto the ball is one of their first experiences of holding. Faced with the offer to let out their weight onto someone else (be it the therapist or a partner) they tend to reply along the lines of: “am I not too heavy for you?” or “I feel like I’m putting you out” or “I don’t like to be touched”. When they are offered the possibility to let out their weight onto the sphere (e. g. through flexion, see Annex Fig. 1), both the client and the therapist can clearly see the zones of tension areas. As they breathe and perceive the contact that the sphere is making, their bodies begin to let out weight. They make comments such as “I felt more relaxed than ever before,” or “I enjoy being here,” or “I never felt so relieved,” among others.
Here we must clarify that resistance to let out weight onto others is an aspect of the client’s history and present that must be worked on. We understand work with the sphere as facilitating a path toward engaging in exploring conflict, not as something that dissolves it. It is especially useful when resistance is too rigid or when a technique poses a risk of re-traumatization.
Softening (toning down): It reverses the relationship between body and gravity in many positions. This reversal, which often causes relief, modifies muscle tone and provides greater possibilities of work with muscles required for static functions, which are generally prone to hypertonia. Therefore significantly reducing muscle tone means an increased ability for proprioceptive realization and a reduction of pain.
Support: The sphere supports movement by functioning as a fulcrum, which increases the possibilities for outward stretching: two opposite points projecting their forces in opposite directions. For instance, when grounding, feet point toward the ground, whereas the ischia point diagonally upward. Stretching helps the client to overcome the boundaries imposed by chronic tension. Although muscle tone is activated, it is aided by the sphere’s support (see Annex Fig. 2). This type of work has proven interesting when working, for instance, with: a) very rigid bodies, because it prevents them from contracting their muscles further, which would increase the tension and b) bodies which are prone to hypertonia, as contact with the sphere has increased proprioceptive realizations, thus making the activation of local muscle tone more effective. As a result of these experiences, both relief and freedom of movement are perceived.
Pushing: By using the sphere, force can be applied according to the client’s muscle tone. Much like the quality of support, this feature allows the client to realize their strength as a vital flow running and projecting itself, and its effects can be seen through the dialog with the sphere’s feedback. One can observe whether these effects are excessive, fitting or insufficient. Our clients have found that it facilitates exploring subjects such as voluntary psychomotor skills and the connection with their energy flow and blocks (see Annex Fig. 3).
Plasticity: The amount of air used to blow up the sphere depends on the type of work one is doing and the client’s psycho-physical profile. In this sense, it is important to observe that a well blown-up ball offers greater resistance, the contact surface on the ground is smaller, it moves faster and demands greater reflex control. One that is less blown-up has a larger contact surface on the ground, it moves more slowly and requires less effort in order to keep balance.
Spheres can adopt the different “tones” of the primary attachment bond: If it is too hard, it ejects the person, as it is harder to keep contact. If it is too “soft”, it provides no holding and feeds back a perception of crumbling. It is interesting to observe the dialog between client and ball in order to figure out the tone that is best fitted for that specific moment in the client’s life.
It allows movement: The client can move by letting out weight when engaged in dialog with the sphere. Actions such as (a) trying to find a balance, (b) sliding, (c) or bouncing help the central nervous system to learn efficiency (Grabner, 2014). Instability, which is a feature of work with the sphere, defies the CNS’s (central nervous system) habitual patterns. This type of work facilitates the exploration of the client’s resources for self-regulation, the acquisition of resources that provide safety and the notion of balance as a constant search rather than a state (see Annex Fig. 4).
Volume: It provides the notion of “content,” thus bringing about the perception of a border and an inner world. Larger spheres give clients the possibility to experience contact with volumes similar to their own. Smaller spheres are used for localized work, and they are useful to reach zones of acute chronic tension.
Texture: We observe that the sphere’s qualities are perceived through the senses in an integral manner. Mario Di Santo (Di Santo, 2012) calls this modality of perception “haptic sensitivity” and defines it as a modality that links touch with other senses (primarily sight and hearing). The characteristics of its material, which is rugged and thin, make it easier for the client to feel it as skin.
Temperature: It is an object that adopts the temperature of the body. Much like the sphere’s texture, its temperature further contributes to the feeling of skin-to-skin contact.
Weight: The weight of larger spheres facilitates designing experiences in which muscle tone is charged and activated. Experiences of charging provide the client with information on what they can or cannot support and the resources they need in order to withstand and contain their energy charge (see Annex Fig. 5).
Ball size: Balls are manufactured in different sizes so that they can be tailored to the client’s therapeutic needs and physical size. We usually use spheres ranging from 20 to 85 cm in diameter.
In the case of larger balls, the right diameter can be figured out with the client sitting on it, with their knees and hips aligned forming a 90° angle (see Annex Fig. 4).
Work can be individual, in pairs or in groups.
Clinical Experiences
In the experiences that follow we aim to describe how spheres were used in our clinical practice. The information detailed here is presumptive and both cases are still ongoing, so it is expected to change when new data is collected (Fréchette, 2013).
Case 1
M (21) shows up for a consult. She is very thin, has short hair and comes across as a small boy. Shortly after arriving she begins to cry, making it harder for her to speak. Later I will find out that her crying is frequent and that if she finds support in our gaze she will calm down and regulate herself.
Her reason for having the consult is a series of almost daily episodes of great anxiety and anguish, which made her feel that she was “leaving” her own body and produced “unpleasant sensations in my head,” and which she found difficult to overcome. Most of the time she was beaten by exhaustion and ended up weary.
She had been living with her boyfriend for two years, having left her mother’s home at the age of 19. She worked sporadically as a photographer and was not studying. Having abundant free time was a source of great worry, which caused her anticipatory anxiety.
Her parents had been apart since she was 8 years old. Her mother (L) has been under psychiatric treatment for over 10 years. M tells me that her mother is a “pill popper,” which hinders communication; thus she finds it impossible to find support in her mother. M was always on the alert due to her mother’s unregulated states, prompting L to phone her daughter at all hours, demanding attention, which left M in a confused state of hatred and guilt that usually resulted in episodes of great anguish.
M used to arrive in the office wearing a smile that would turn into sobbing as soon as she sat down and relaxed on the couch. Due to her difficulty in letting out words, slowly and together we managed to figure out the reason for such anguish. As her body had a tendency to come undone, we started every session with her lying down. I would call out parts of her body and she would fill them with sensations upon hearing my voice. In this sense the ball was – and still is – great company for us both. Lying down, she would travel the length of her body using a medium-sized (50 cm) semi-inflated ball, marking out her borders in order to sensorially tell her inside from her outside (see Annex Fig. 6). M would call this moment “coming back to me” (to herself). I observed (and she felt) how her pale skin would turn rosy and how her limbs would become warmer.
Slowly she managed to work on deeper muscle layers. Lying face-up and forming a 90° angle with her legs, her feet on the ball, she would use her soles to push the large (80 cm) sphere set against the wall, which offered resistance (see Annex Fig. 7). With this process her voice would come out, at first inaudible, it would turn ever clearer, taking turns appearing and disappearing. On other occasions, she would stand up and hold the medium-sized ball by the sides at chest level, pressing it inwards using the muscles in her arms with a protruding jaw. As she did so, some anger was beginning to crop up (see Annex Fig. 3). At times when rage would begin to activate, she would quickly crumble and state, “I have no strength left” or “I’m not angry anymore,” thus letting her resistance show. As the bond became a foundation for safety, I encouraged her to stay in those “discomfort zones” that her anger led her into.
“Leaving” was one of her most usual defenses, but it was becoming inefficient. It was therefore interesting to observe what happened over three years with respect to grounding. Initially, when grounding she would quickly get out of the position in the space of a few seconds, because the feeling in her feet would prove unbearable, as she would barely feel them. When I observed this difficulty, I offered her a medium-sized semi-inflated ball to place on her anterior hip, so that as she released her upper body downward, her belly would be resting on the ball, which would in turn remain between her abdomen and her thighs (see Annex Fig. 8). The weight of her organs would thus be let out onto the sphere, making it more supportive and, at the same time, increasing the proprioceptive realization that her pelvis was becoming loose and functioning as a ground connection. Gradually M would tolerate the sensation for more and more seconds. Now she enjoys her ground connection, letting out the weight of her head and trunk, supported only by her feet and legs.
At first, due to her tendency to “leave”, I had presumptively diagnosed schizoid disorder. The “unpleasant sensations in her head” tore her apart from her body and took hold of her neck, straining it. We spent entire sessions working on that strain ring. M would lie down face-up and I would place a small (20 cm) ball under her cervical vertebrae so that her cranium, feeling a firm sensation of holding, would smoothly let out its weight on to the ground. By making subtle movements sideways and up and down, and alternating these with moments of stillness, M would begin to feel more whole. Other clients who underwent the same experience have provided similar feedback (see Annex Fig. 9).
Halfway through our first year together I suggested that she consult with a psychiatrist. She found it very difficult to live her daily life, and I felt that alone I could not help her overcome this, as two weekly meetings were insufficient. Her first reaction was one of fear and rejection. M was afraid of “becoming” her mother, which is why the mere talk of psychotropic drugs brought that identifying idea into her imagination. However, thanks to M’s trust in me, we were able to include a psychiatrist on our team. All three of us worked together for almost a year. After 6 months of treatment, the dose of her medicine (a blend of an antidepressant and an anxiolytic) was gradually reduced until she no longer needed it. At this point, we were able to work at a different pace.
Her mother’s dominance in our sessions began to dwindle, and other issues and possibilities arose. L kept demanding her presence, but M was stronger to face the situation and say no. Her anger scares her less and less, and she can safely express her violent impulses by tolerating stronger charges within the borders of her self. In this sense, having the ball as mediator and not showing her teeth directly to me was highly useful. As it is large and soft, being able to hit it and kick it without hurting herself or me was particularly helpful for expressing her emotions (see Annex Fig. 10).
At times some marks of schizoidal mechanisms appear when some of her disintegration and division crops up. However, her struggle to keep an integrated self without merging with others and her difficulties setting limits, to contain her charge and to ground – and therefore to inhabit her own body and be present – lead me toward a presumptive diagnosis of borderline structure.
In spite of all the difficulties we have elaborated to date, M has taken a 180° turn. Her muscles have toned up, she walks more firmly and the pitch of her voice is lower. She has taken up yoga and astrology. She got a stable job and amicably separated from her partner. She dared to move in with a friend and, when that did not turn out, took it upon herself to find a house to live in on her own. When I met her she was like an unresourceful child and now I see an independent woman that can fend for herself and even ask for help when she needs it. Sometimes we meet every week and sometimes we meet every other week. She can come and go as she pleases from her sessions and therefore come and go with a more flexible and healthy bond.
Case 2
F comes for her consult having had Bioenergetics and Esferodinamia classes. She requested my phone number at IAAB because she knew I worked with spheres and was interested to see how a therapeutic process using such items might work.
Over our first interviews I observed that F (27) was tall, of medium build and voluptuous. Her face gestured a lot and she bit herself and touched her mouth insistently. She spoke very loudly. Her tone of voice appeared to make up for her lack of muscle tone. Even though her body seemed to be charged, she sat on the couch as if crumbling. Her gaze hungered for contact but at the same time she found it hard to keep eye contact with me. Emotionally she seemed troubled by her inability to let go of her relationship with a former partner. Her demand to me was that she needed help to “end her breakup.”
Over our first year of treatment I realized that F attempted to make contact with me but did not fully trust the therapy. It seemed as if she suspected that she might be betrayed at some point. Perhaps she thought I would lose my practice as a therapist to establish a regular relationship, as had occurred with a previous therapist. I suspected that made her think of a certain “illegality” and promiscuity, a feature of some of her ongoing relationships. Over the course of our therapy it transpired that it was also linked to her family history.
F is the second of four children. She has been living alone since she was 26. Her living depends largely on her father’s contributions. Her father still gives her a monthly allowance and monitors her earnings and expenses.
It was a real challenge to map out F’s history. At first she would miss sessions or arrive late. She claimed to acknowledge being a “ghost,” i. e. disappearing without so much as a word of explanation. She sometimes said that she intended to show up but when the moment came she could not. It seemed that some of her resistance was present by being absent without being aware of it at all. After a year, I began to voice how I felt about these attitudes so that we might make sense of them together based on her history. Consequently, through F’s bond and therapy she was able to link those events with childhood experiences that she was defending herself from. She had an emotionally unstable mother and a father with psychopathic traits and a severe judgment of F that turned her into the object of both her parents’ childish needs. Insufficiently equipped to assert herself and showing signs of confusion, F could not question her parents, who she claimed “had given her everything” and consequently could not bring herself to understand why “she could do almost nothing” (internally echoing her father’s severity and her mother’s strive for perfection). Using money to manipulate her, her father still disables her. Her mother, who has difficulty keeping in touch, fluctuated between merging with F and leaving her all by herself, so that F was unable to understand the changes from one state into another. As an adult, when she shows any signs of questioning her family’s dynamics, the family goes silent and will lash out at her in an airtight complicity that turns her into the black sheep of the family. This is true even though it is clear that there is conflict; for instance, her father is in an ongoing affair with the housekeeper, who has been working for them for a long time and lives in the same house.
I presume that F’s history includes elements of a borderline structure that provided her with insufficient defensive resources to confront the inner struggle between her anxiety when she was alone and her difficulty trying to make contact. The intimacy of a balanced and safe attachment bond to create a healthy self appeared to be an alien experience.
Some Notes about the Therapy
When F was first invited to work with her body, she claimed to perceive it as uninhabited. She felt it shamed her and exposed her to harsh judgment. Proposals were initially aimed at helping her to consciously make contact with her body, inhabiting it through breathing. She found the sphere reliable and it seemed that it helped her to protect herself from me (that is, aspects of her parents projected onto me). It allowed her to set a much-needed limit but she was not able to set it when she was by herself. Kneeling behind the sphere, her chest making contact with it, she was able to breathe and hide her body behind it so that there would be something “between” herself and me (see Annex Fig. 11). In other words, it became a border allowing her to differentiate herself from me. By repeating these experiences she began to recognize herself in her breathing, as air would block in her throat, disconnecting her head from the rest of her body. She could feel neither her pelvis nor her legs. She felt disorganized in her movements, which was apparent. We both observed how hard it was for her to make eye contact, and how she was uncomfortable with her eyes closed. Through these emerging realizations, we managed to gradually construct a realization of her that was based on a configuration I provided and which she became more and more able to adopt.
As the process rolled on, she managed to climb on to the sphere in what was previously called a “flexion.” There was already “more body” and the sphere provided a foundation for safety (see Annex Fig. 1).
At first exercises were aimed at letting her perceive the weight of her body, the places that were and were not in contact, the ball’s feedback of her breathing gesture, what it was like to be held by the sphere and how she was able to move as her feet and hands began to push. I joined in by keeping a certain distance from F or by lightly touching her in order to either reinforce her grounding or increase her realization of different parts of her body. Both pushing and her contact with the sphere and myself were aimed at constructing more accurate borders and reinforcing her grounding.
F reported that she enjoyed being there, feeling held by the sphere. She was dancing with the sphere and would only let go when she had had enough. She was able to make decisions, such as asking me to work with the sphere and anticipating when to start and end contact, something that had not occurred with her mother.
The bond between her, the ball and me was gradually strengthened. Gradually and patiently I constructed myself as a foundation for F’s safety. An important moment in the process was when she was flexing and I felt I could stay next to her, rocking her on the sphere and inviting her to make eye contact with me whenever she wanted to and was able to. F was moved and was surprised to be able to do so. She said she had no recollection of ever being looked at in that way. She described my look as sweet, warm and “being there,” unable to use more terminology (perhaps there were less words because it was a primary realization). We understood that she was trying to convey she did not feel pushed or invaded. It calmed her down instead of causing her anxiety, which occurred whenever other people looked at her. Such anxiety frequently makes her feel inadequate in her relationships, and she works hard not to repeat her family’s stigma, which has burdened her with the responsibility for “ruining everything.” Thus the realization that she could bond and feel calm, differentiated and able to regulate herself helped her feel that this might be true in other relationships she currently has, using the resources she now has as an adult.
Building trust and safety in our bond was the first step toward exploring her full capacity for self-support and self-regulation. The sphere offered a place of safety on this road. She has recently arrived at one of our sessions celebrating our two years since starting the process and grateful to me for helping her to keep it up. I underscore this because I consider that such emotions have helped to heal her previous model of bonding where the feeling of inadequacy, of being in debt and feeling insufficient prevailed. We are currently working on her self-support. During this stage, the sphere’s holding is less needed, as she can be sitting and focusing on activating her legs and her center through bouncing (see Annex Fig. 4). A recent experience that we are still exploring is standing up from the ball and observing the sensory and emotional echo that is activated and the senses in connection with her history.
Today F can handle her own money and lives with a stable partner. I consider that the great contribution of the sphere to F’s therapy was primarily building trust between us, making it easier to construct a bond and leaving room for our creativity to discover how to write new lines in her present and veer away from the single story, thereby regaining a sort of lost paradise.
Conclusions
In the course of our training, as well as in many fundamental readings, we have learned how to work with some classic techniques and objects such as the Bioenergetic stool, the mattress, the racket and the towel (Krsul & Dosoretz, 2007).
Based on our research discoveries, we postulate that these uses of the sphere may be another new and essential tool in a contemporary Bioenergetic therapeutic setting.
The sphere is felt as a motherified object insofar as it provides safety and tenderness, helping with empathy and aiding the client and therapist with the discovery of vital bonds.
We hope that this piece will be a contribution for colleagues who seek to begin using spheres or an invitation to widen the scope of their use.
Footnotes
- [1]
- Our work with spheres is validated by Escuela de Esferobalones, coordinated by Anabella Lozano. www.esferobalones.com/ Esferodinamia Reorganización Postural. In English: Dynamic Sphere Postural Reorganization.
- [2]
- Alma Falkenberg, an Italian dancer who taught in Argentina and introduced Contact Improvisation to the country. It is from this dance technique that he began the exploration of what he patented as Postural Reorganization Spherodinamia.
- [3]
- Esferodinamia RP is inscribed within the Somatic Education field. According to its creator, Tomas Hanna, Somatic Education is a field that uses an integral approach centering on the body to help people achieve a sense of wholeness, and to transform themselves through movement and certain sensitization practices that aim to create psychological and physical well-being.
- [4]
- In Bioenergetics, such qualities are rhythm, synchronization, support, affective tuning, regulation of sensory and emotional states, configuration of sensory and emotional experiences, representation and mending. (Tonella, 2011)
References
Adichie, C. (2009). Chimamanda Adichie: The Danger of a Single Story [Video file]. Retrieved from www.ted.com/talks/chimamanda_adichie_the_danger_of_a_single_story.
Di Santo, M. (2012). Amplitud del movimiento. Buenos Aires: Paidotribo.
de Souza Soares, M. C. Auto-conhecimiento, prazer e alegría a través das bolas terapéuticas. Retrieved from libertas.com.br
Dolto, F. (1986). La imagen inconsciente del cuerpo. Barcelona, Buenos Aires, México: Paidós.
Fauser, W. (2015). The Importance of Integrating. Pre-and Perinatal Issues into Bioenergetic Analysis. Bioenergetic Analysis. The clinical Journal of bioenergetic analysis Vol 25. Germany: Psychosozial-Verlag.
Fréchette, L. (2013). Creatividad y diagnóstico. Observando la expresión única en la persona. Bibliography for the Certified Bioenergetic Analyst training program at the Instituto Argentino de Análisis Bioenergético. Buenos Aires.
Fréchette, L. (2013). Temas y estrategias de trabajo con cada carácter: algunos puntos de referencia. Bibliography for the Certified Bioenergetic Analyst training program at the Instituto Argentino de Análisis Bioenergético. Buenos Aires.
Freud, S. (1988). El malestar en la cultura. Buenos Aires: Alianza Editorial.
Grabner, L. (2014). Introducción a la Neurosicoeducación. Neuroplasticidad y redes Hebbianas. Las bases del aprendizaje. Buenos Aires: Asociación Educar para el Desarrollo Humano.
Krsul, A. (2013). Psicocorporalidad: el cuerpo nunca está afuera. Retrieved from www.bioenergetica.org.ar
Krsul, A. & L. Dosoretz (2007). Algunas reflexiones sobre la utilización de herramientas clásicas en el proceso bioenergético. Retrieved from www.bioenergetica.org.ar/inicio/wp-content/uploads/2015/10/Algunas-reflexiones-por-Ana-Krusl-y-Liliana-Dosoretz.pdf.
Lowen, A. & L. Lowen (1990). Ejercicios de Bioenergética. Málaga: Sirio S. A. Lowen, A. (1997). Alegría – La entrega del cuerpo y la vida. Sao Paulo: Summus.
Lozano, A, J. Cegatti & S. Martínez (2012). “Educación Somática”. Rosario, Argentina: In Actas del I Encuentro Latinoamericano de Investigadores sobre Cuerpos y Corporalidades en las Culturas. Editorial Investigaciones en Artes Escénicas y Performática.
Tonella, G. (2013) La Construcción de la Continuidad Psicocorporal. El sí mismo. Bibliography for the Certified Bioenergetic Analyst training program at the Instituto Argentino de Análisis Bioenergético. Buenos Aires.
Tonella, G. (2011). Le corps et l’analyse. Vol 12. In Revue francophone d’Analyse Bioenergétique.
Tonella, G. (2006). Los patrones de apego. Bibliography for the Certified Bioenergetic Analyst training program at the Instituto Argentino de Análisis Bioenergético. Buenos Aires.
Winnicott, D. W. (1972). Realidad y Juego. Buenos Aires: Granica.
Abstracts
German
In diesem Artikel stellen wir eine “Biosphärenpraxis” vor. Sie ist aus der Integration unserer Erfahrung in Bioenergetischer Analyse mit “Dynamic Sphere Postural Reorganization” (EsferodinamiaReorganización Postural, hier im folgenden “RP” technique genannt) entstanden. Wir beschreiben die Eigenschaften der Sphäre (großer Gummiball) und wie die Sphäre im Rahmen körperpsychotherapeutischer Interventionen hilfreich sein kann. Abschließend betrachten wir zwei Fälle, die dieses klinische Werkzeug benutzen. Die Sphäre wird zu einem Element, das klinische und erzieherische Arbeit in zeitgenössischer Bioenergetischer Analyse erleichtert.
French
Nous présentons dans cet article ce qu’est la pratique des « Biosphères ». Cette pratique a été développée en intégrant à notre formation en analyse bioénergétique la « Réorganisation posturale par l’utilisation dynamique de la sphère » (Esferodinamia Reorganización Postural, que nous appellerons technique “RP”). Nous décrivons les qualités de la sphère (gros ballon de gym) ainsi que la façon dont elle peut nous aider dans nos interventions thérapeutiques psychocorporelles. Enfin, nous présentons deux vignettes cliniques utilisant cet outil. La sphère constitue un élément qui facilite le travail clinique et éducatif dans le cadre de l’analyse bioénergétique contemporaine.
Italian
In questo articolo intendiamo presentare il lavoro “Biospheres”. Questo si è evoluto in conseguenza dell’integrazione della nostra formazione in analisi bioenergetica con la “Dynamic Sphere Postural Reorganization” (Esferodinamia Reorganización Postural, cui faremo riferimento con la sigla “RP”). Descriviamo le qualità della sfera (grande palla di gomma) e come può essere utile per interventi di psicoterapia corporea. Infine, esaminiamo due casi utilizzando questo strumento clinico. La sfera diventa l’elemento che facilita il lavoro clinico ed educativo nel campo bioenergetico contemporaneo.
Portuguese
Apresentamos, neste artigo, a prática da “Biosfera”, que evoluiu como resultado da integração das nossas experiências formativas em Análise Bioenergética com a reorganização dinâmica da esfera postural – Esferodinâmica da Reorganização Postural -à qual nos referiremos como técnica “RP”. Descrevemos as qualidades da esfera (grande bola de borracha) e como ela pode auxiliar quando fazemos intervenções, na psicoterapia corporal. Finalmente, examinamos dois casos onde essa ferramenta clínica é utilizada. A esfera torna-se um elemento que facilita o trabalho clínico e o educacional no campo da Bioenergética contemporânea.
Russian
Представлена практика биоэнергетической работы с фитболом – большим эластичным шаром, используемым для фитнеса, названным «биосферой» по аналогии с «биоэнергетическим табуретом». Эта методика появилась в результате объединения знаний, накопленных в Биоэнергетическом Анализе и в методе коррекции постуры (осанки и других паттернов поддержания определенного положения тела) при помощи баланса на неустойчивых, динамических поверхностях (Esferodinamia Reorganización Postural, или «техника RP»). Определены требования к качеству фитбола, а также показано, в чем эта методика может быть полезна в телесной психотерапевтической работе. В заключение рассматриваются два терапевтических примера использования «биосферы». Биоэнергетическое применение фитбола становится инструментом, который может оказать значительную помощь в терапевтической и образовательной деятельности в современном Биоэнергетическом Анализе.
Abour the Authors
Julia Cegatti attended Buenos Aires University where she developed as a psychology teacher and researcher. She is currently completing her studies as a bioenergetic analyst at the Argentine Institute of Bioenergetic Analysis. She works as a therapist in Buenos Aires, Argentina. Julia is an instructor and a member of the teaching staff at the Esferodinamia School of postural reorganization, an institution in which she was trained in this technique.
Leticia Polosecki received a degree in psychology at Buenos Aires University and is a Certified Bioenergetic Analysis Therapist (CBT). She is a teacher at the Argentine Institute of Bioenergetic Analysis and is an instructor of Esferodinamia postural reorganization. She has participated for 5 years in study groups in biosynthesis. Currently Leticia is in her first year studying the formation of somatic integration at the Center for Research and Study of Corporal languages and techniques. She practises as a therapist and teacher in Buenos Aires, Argentina.
Since 2010, Leticia and Julia have been exploring the integration of Esferodinamia postural reorganization with bioenergetics for teaching and clinical purposes.
Annex

Fig 1: Flexion. Feet and hands on the floor. The rest of the body lets its weight out onto the sphere.
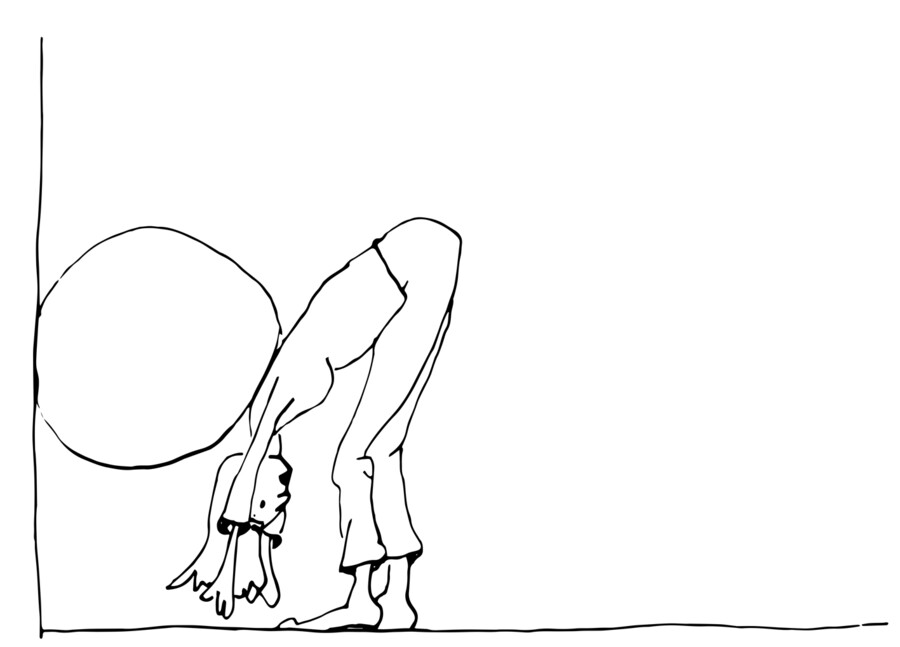
Fig 2: Grounding with 80 cm sphere as back support against the wall.
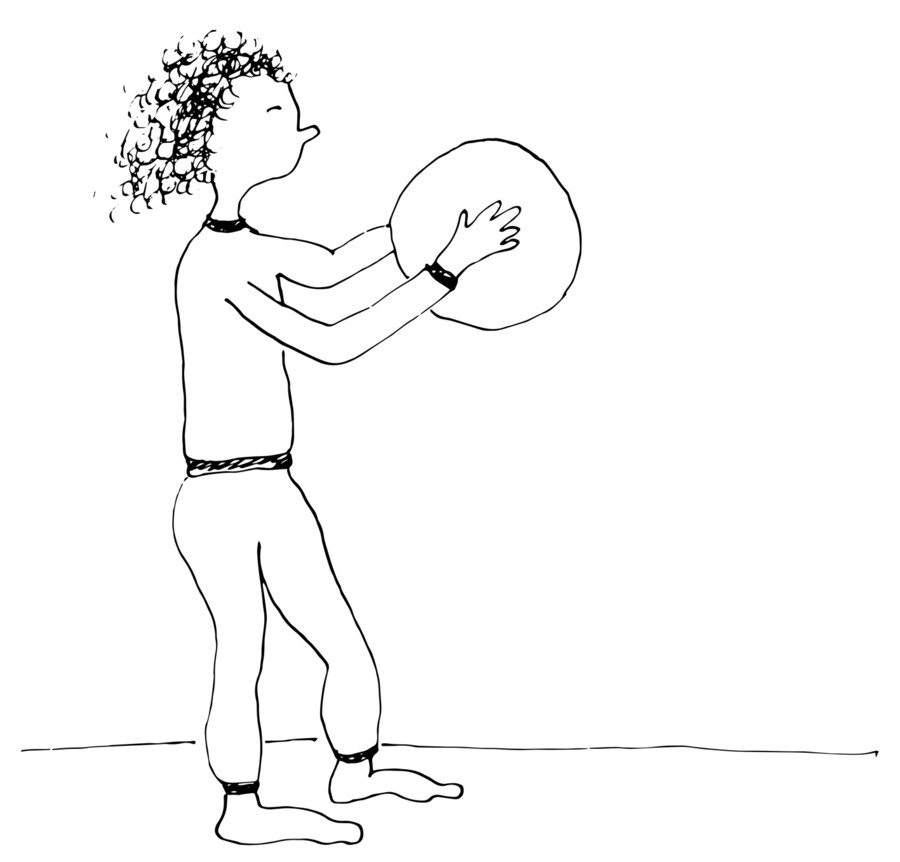
Fig 3:Hands pushing on a 50 cm sphere at the chest level.
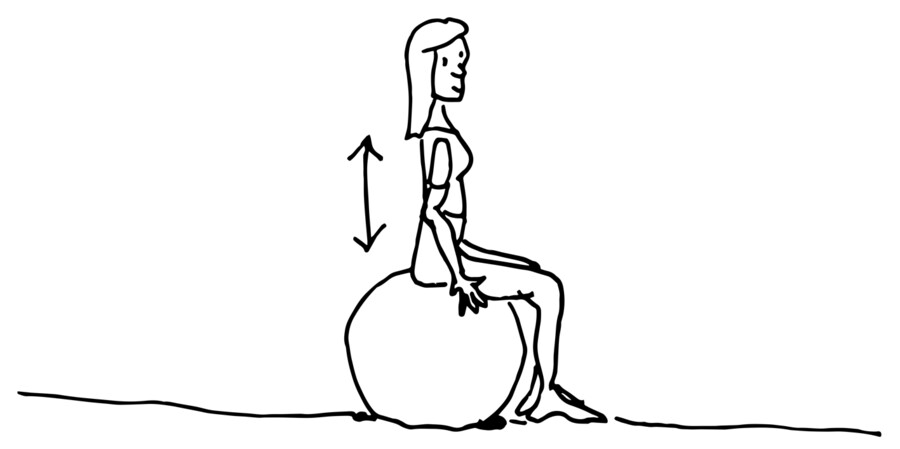
Fig 4: Sitting on an 80 cm sphere. Bouncing from the soles pushing on the ground, using the center of the sphere as support and projecting the top of the head toward the ceiling.
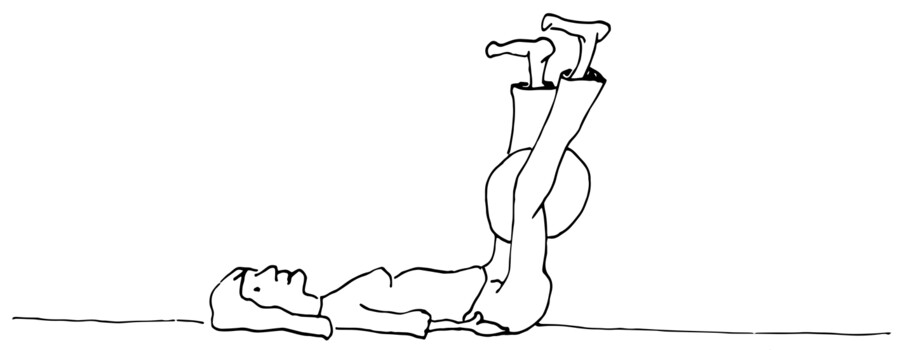
Fig 5: Holding a 50 or 80 cm sphere, depending on the charge required. Lying down with the sphere placed between the legs. To further activate the tone, slightly push with adductor muscles toward the center of the sphere taking care not to lock the knees.
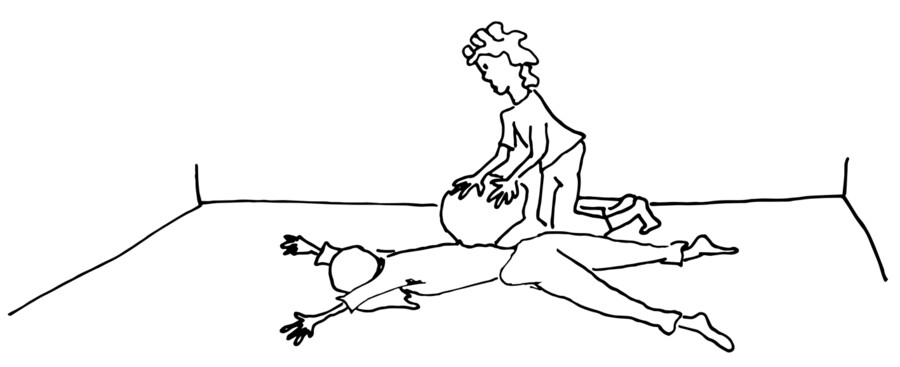
Fig 6: Transfer of weight by the facilitator with 50 cm semi-inflated sphere. The person receiving the weight is lying on a comfortable, albeit not very soft, surface.
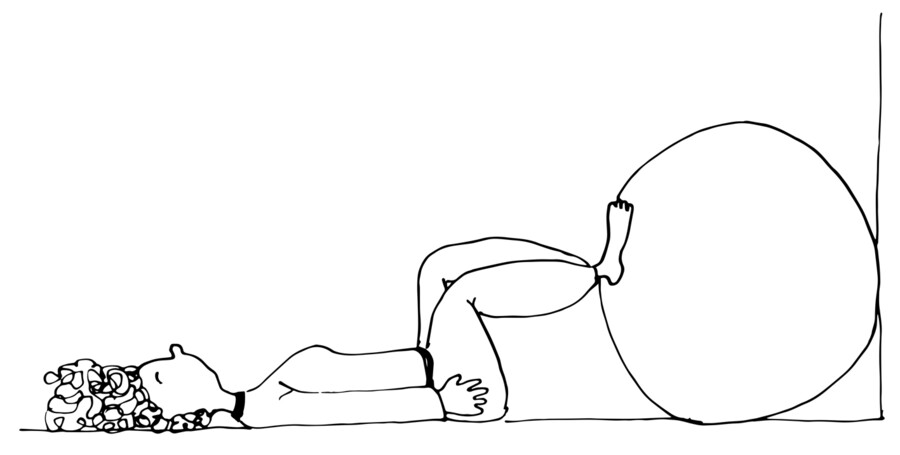
Fig 7: Soles pushing on an 80 cm sphere set against the wall.
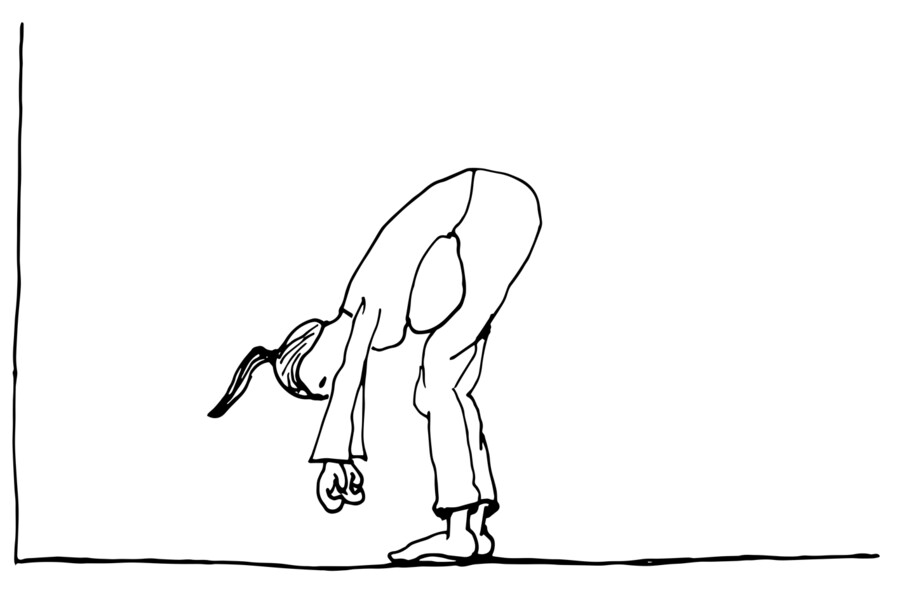
Fig 8: Grounding with 50 cm semi-inflated sphere placed between the pelvis and the abdomen as if it were an apron.

Fig 9: Lying down with a 20 cm sphere on the cervical vertebrae.
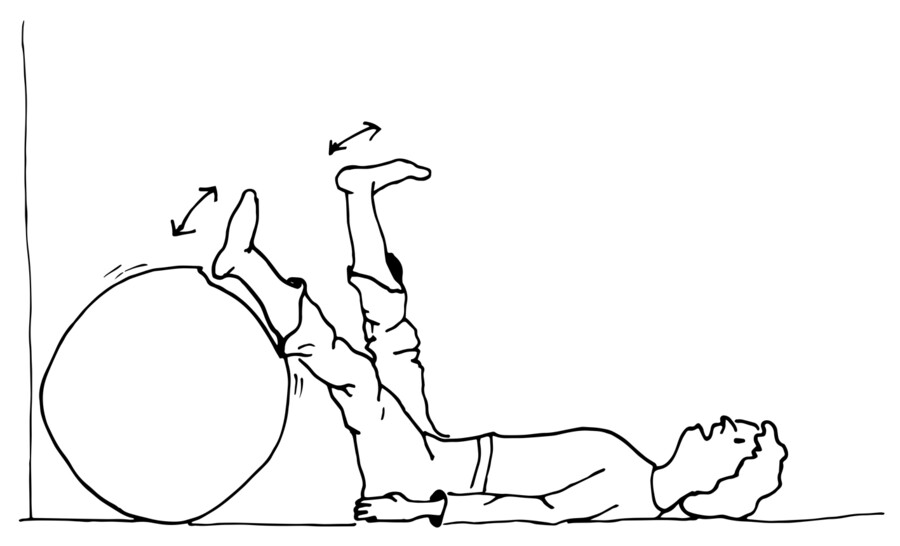
Fig 10: “Kicking” against an 80 cm sphere set against the wall.

Fig 11: Kneeling behind an 80 cm sphere with the chest on it and the head drooping to the side.