Aggression as a Significant Factor in the Formation and Expression of the Self
Anat Gihon
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2018 (28), 75-97
https://doi.org/10.30820/0743-4804-2018-28-75 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstract: Aggression, in the broad sense of the term, is examined from psychoanalytic literature with a focus on Bioenergetic theory and treatment. Clinical material enhances the exploration of working with aggression in patients, including energetic work with breath, grounding, boundary setting and expressive movements. This paper explores dealing with aggression when working with weaker structures, while working from a relational matrix and when encountering issues of countertransference.
Key words: Aggression, moving towards (approach), vitality, sexuality, reaching out, assertion
Introduction
In his monograph, Aggression and Violence in the Individual, Alexander Lowen reminds us that although the popular meaning of aggression is connected with hostility and even violence, “from a point of view of personality, aggression is contrasted with passivity”, and its actual meaning is “to move forward, towards”. (Lowen, A. 2005, p. 297)
When talking about aggression in this paper, I see it as a sequential libidinal charge correlated with the muscular system. It is rooted in breathing, which is the very core of voluntary pulsatory movement. When given enough available energy, aggression starts from the capacity to want and initiate a movement towards contact with the outside. It is the force that takes us forward in life, reaching out for fulfillment of our needs and wishes, (ibid., p. 297) and of overcoming obstacles for such movement. Aggression includes assertion, it fuels the ability to set and claim boundaries, protecting the self’s integrity in part by feeling and expressing anger. In healthy development, aggression, along with other factors such as grounding, plays a central role in building a well balanced, well bounded, well-regulated container for oneself. All of the above are actually connected with self-possession, self-expression, self-assertion (Lowen, A. 1983, p. 111–112), and with self-respect, (Helfaer, P. 1998, p. 55) which are necessary ingredients for the formation of a healthy, true self, and for maintaining respectful relationships with others.
Since staying in relationship with the parent is the deepest existential need for a child, when aggression, at least in the child’s mind, poses a threat to the existence of contact with the parent, aggression will often be blocked by fear, finding alternative avenues, turning against the self in different ways, and/or be expressed in destructive manners, like in criticalness, rage, hate, perversion or violence. (Appendix 1, based on Hilton, R. 2007, p. 167). This will affect the life of the individual in almost every aspect.
Every significant encounter between two people – any two people – is actually an encounter between two bodies – two selves, with unique adaptive organizations, folding within them a unique history of physical, mental and emotional experiences. Every such encounter stimulates the authentic life movement, the adaptive–defensive organization and a cluster of bodily-emotional-mental memories, often of traumatic experiences, all of which will affect the quality of this encounter. This is true about our encounter with everyone, including with our patients, and can actually be seen as the energetic base for transference and counter-transference. This is an element that we should be aware of when we have to help our patients re-find their authentic movement. Since aggression was stopped because it lacked the needed environmental response, positioning ourselves in relation to our patients with the needed attunement is crucial for the therapy to work well. Still, being recipients of such charge, like anger, rage etc., can evoke our own historical traumas, especially if, like in the lives of many of us that chose to become therapists, our traumas have some similarities to the relational traumas of our patients. This is especially true of those of us therapists who have had to serve in some way or another as care takers of our parents.
Theory of Aggression in Psychoanalysis
The meaning and perception of aggression in the psychoanalytic literature is widely varied. I will not go into the many points of view regarding the nature and role of aggression that have developed with the development of psychoanalytic thinking. The majority of writers view aggression as synonymous with negative affects such as rage, hate, violence, destruction, perversion, sadism, envy, and revenge. On one end of the spectrum it was perceived as an innate, primary, and destructive drive (Freud, Klein and others). Freud even perceived it as the representation of the death drive. On the other end of the spectrum, with analysts like Kohut or other Self Psychologists, it was seen not as an innate force, but as a response to disturbances of the self, in particular with persistent empathic failures by the person who occupies the function of the selfobject, or as a defense reaction to humiliation and injured narcissism. (Rizzuto, A. M. Meissner, W. W. Buie, D. 2004, p. 5)
Others, such as Reich and later Lowen, Winnicott, Rizzuto, Meissner and Buie, have classified aggression as an innate force, serving significant psychic and developmental needs. In this paper I chose to relate mostly to the perception of Reich, Lowen, and Winnicott who in looking at aggression, focused on the energetic point of view, associating it with movement and vitality.
In The Function of the Orgasm, written in 1942, Reich, looking at aggression from the point of view of drive theory, relates it to liveliness, rooted in sexuality:
“Aggression, in the strict sense of the word … means ‘approach’. Every … manifestation of life is aggressive, the act of sexual pleasure as well as the act of destructive hate, the sadistic act as well as the act of procuring food. Aggression is the life expression of the musculature, of the system of movement … [and] is always an attempt to provide the means for the gratification of a vital need.” (Reich, W. 1973, p. 156. emphasis added)
The more negative aspects of aggression, like destruction, perversion and especially hate, are in Reich’s view a result of blocked sexual charge:
“If aggressive sexuality is denied gratification, the urge to gratify it in spite of the denial continues to make itself felt … the impulse arises to experience the desired pleasure at all cost. The need for aggression begins to drown out the need for love … Hate develops as a result of the exclusion of the original goal of love … and it is most intense when the act of loving or being loved is blocked. This is what brings the sexually motivated destructive intention into the aggressive action.” (ibid., p. 156.)
In subsequent years, with psychoanalytic theory shifting some of the focus from drive on to early attachment, the view of the roots of destruction, rage, hate, and even of violence were shifted. Psychoanalytic theory moved from viewing the roots of destruction as pure blocked sexuality, to seeing its source in failures of attunement by the significant others in the infant’s environment. That failure by those in the child’s environment can take the form of an empathic failure or missed attunement; or a behavior that humiliates and diminishes the child; or some impingement on the child that violates boundaries. It can also come out of the child’s identification with the destructiveness in the parent and the introjections of the destructive forces present in the parent.
Lowen’s formulation of aggression leans on the verbal meaning of the words “moving forward, or towards”. “We consider someone to be aggressive when he moves out or reaches out for the satisfaction of his needs” (Lowen, A. 2005, p. 297) and for pleasure (ibid., p. 299). Breathing, sucking the nipple, reaching out for contact, as well as assertiveness, boundary setting, expression of anger, and sexuality, are all considered aggressive functions (ibid., p. 299, 302).
In his early work Lowen made a distinction between aggressive and soft moving out for contact, associating the latter with longing which “is characterized by the movement of excitation along the front of the body, while aggression results from the flow of excitation into the muscular system, especially into the large muscles of the back, the legs and the arms, which are involved in the action of moving towards.” (Lowen, A. 1958, p. 79, 81)
In a way, Lowen’s definition goes back to basics by identifying the deepest element of human aggression with the very core of human pulsatory movement, that of expansion into contact with the outside.
I believe that we can see aggression as the charge that fuels any moving out, even the soft, tender movements of reaching out for contact. As we will see later in a clinical case, when people are profoundly injured all the way to their core, even the slightest initiation of reaching out for contact is very difficult for them. We can thus say that the way life is in our body is a dialogue between soft and more forceful movements but that some aggression, at least in the form of full breathing, is needed also for the soft movements to flow.
Winnicott’s view of aggression is not very different than Reich’s definition.
Dr. Osnat Ere’el, an Israeli psychoanalyst, describes Winnicott’s attitude to aggression in the introduction to the Hebrew translation of his article, Aggression in relation to emotional development1. Using energetic terms, she states that, “Winnicott sees aggression as the fire within us; as the engine, the developmental energy, finding its expression in activity, appetite, movement, spontaneity and love.” (Ere’el, O., in Winnicott, 2009 p. 92).
Rizzuo, Meissner and Dan Buie use energetic and motivational terms when presenting their perception of aggression. According to them, “aggression is a biologically-rooted capacity … of the mind to carry out psychic or physical activity directed to overcoming any obstacle interfering with the completion of an intended internal or external action.” (Rizzuto, A. M. Meissner, W. W. Buie, D. 2004, p. 69, 104).
We can thus see aggression as the force that serves as a vehicle for initiation and expression, moving people toward fulfillment of authentic wishes, toward contact with the outside and toward self-fulfillment. Aggression is the charge that supports the expression of a true, contactful self. It is also the charge that helps us push away or aside an obstacle that interferes with those actions. We can see it as assertiveness, which is the ability to express our needs and wants with clarity and force, as well as the force that helps us set a boundary, supporting our separateness, individuality and self-containment. Aggression supports direct expression of frustration and of anger, which are natural responses to situations that injure or threaten the individual’s integrity, his freedom, both emotional and physical and his self-respect. Both Reich and later Lowen saw anger as an important life-positive force in the lives of all creatures, which has strong healing, restorative and protective properties.
When the flow of aggression is blocked or being sabotaged, the charge will either turn in against the self, and will often be experienced as self-hate, shame, and guilt; and/or it will accumulate, being expressed outwardly, in a destructive force such as rage, hate, and violence.
When we look at humans we see two essential inherent and interwoven movements. The first is from the core outward, toward the envelope of the body and out to the world, moving for the satisfaction of a need. This fits Lowen’s basic definition of aggression. The other movement is on the longitudinal axis, one of letting down, letting go, going with gravity, being supported by the ground, which is what the grounding pulsatory wave is about, “the enabling of a longitudinal wave to stream through the body”, enabling “oneself to experience itself fully in relation to a base of support” (Lowen, A. 1975, p. 195). There are always interrelationships between aggression and grounding – every movement toward the outside needs a “ground” to lean on. In relational terms, it needs an “other”.
This dialogue between the movements from the core out with the movement of letting down can be seen as the core of pulsation. In optimal conditions the organism extends itself, expands toward contact with the outside with the exterior parts of the body; then it retreats inward, to digest that encounter. It lets down into itself, rests and at a certain point when ready, and only then, moves out again toward contact with the outside. We can say that this very simple description is actually the biological basis of the life of an authentic, well-regulated self, one that is moved from within. This is also a simple description of the energetic base of healthy relations with another. When the regulation of moving or reaching out, or of retreating is prohibited or made impossible, this becomes the basis for the creation of contactlessness (Reich, W. 1972, p. 311), the state of needing a false presentation of self. This false self is experienced by the person as real despite the inability to be spontaneous. It is analogous to what Winnicott referred to as a False-Self formation.
Theory of Anger and Rage in Bioenergetics
In his book Joy Lowen says, “Anger is an important emotion in the life of all creatures, since it serves to maintain and protect the physical and psychological integrity of the organism … Without anger one is helpless against the assaults to which life subjects us” (Lowen, A. 1995, p. 103). Like any other mammal, without the option to experience anger we might freeze in fear. In traumatic situations, this is the fighting part of the “fight and flight” reaction.
“The infant young of most developed species lack the motor coordination necessary for the expression of anger, and need the protection of parents. This is especially true for the human infant, who needs a longer time than other mammalian infants to get this ability” (ibid., p. 103).
In the same book Lowen is reminded of a statement of Reich from a seminar given by him in1945, where Reich said:
“Neurotic personality only develops when a child’s ability to express anger at an insult is blocked … when the act of reaching out for pleasure is frustrated, a withdrawal of the impulse takes place, creating a loss of integrity in the body. The integrity can be restored only through the mobilization of aggressive energy and its expression as anger. This would reestablish the organism’s natural boundaries and its ability to reach out again” (ibid., p. 104).
In order to have a body that can express anger freely, one has to have a ground to develop it from. That ground starts with another attuned, empathic present body, that can not only be there for the developing infant in ways needed, but that can sustain the expression of anger in its growing complexity, without contracting or withdrawing in reaction to it.
The ability to contain anger is the counter-part of the ability to express anger effectively. With becoming a member of society and the development of social skills, other than the capacity for self-expression, the capacity for regulating that expression, i. e. of containing, should develop.
When anger is blocked, because of external or internalized negation, (see appendix b. Bob Hilton’s graph, adapted by the author), it is accumulated in one’s body, having to find bypasses, often not conscious to the individual. The charge never disappears. It either turns against the self – in self hate and negation systems like guilt, shame, anxiety, inferiority, and/or masochism; or it turns into rage, destruction, hate, violence, sadism and abuse. Very often both movements happen. Rage does not explode in reaction to an immediate, realistic stimulus, but often in response to a stimulus that reminds one of previous situations, that is a response to capsulated body-memory. We can actually see it as an aspect of transference. Often it is a reaction to what is experienced by one as empathic failure. Kohut relates to narcissistic rage as an expression towards a disappointing self-object. Very injured people can feel rejection and rage in the face of the slightest separateness from the other, which is often found in people that have gone through traumatic experiences.
Unlike anger, rage is a destructive emotion. It is intended to hurt, to break someone or break something. In his book, Toxic Nourishments, Mikel Eigen gives a very vivid picture of what rage feels like:
“The rage in one’s life is cumulative. It sediments in the belly of one’s being and corrupts muscles, nerves, and veins. It not only stiffens one’s body, it poisons one’s thoughts. One bears grudges from early childhood on, so that one is ready to jump on others for small things … The chronic outrage over injury can eat at life like an acid and corrode psychosomatic integrity.” (Eigen, M., 1999, p. 48)
The Role of Aggression in Early Development
Look at humans: from before conception, with the sperm rushing for the egg, through the active movements of the embryo, pushing/being pushed out to the outside world in labor, with the first aggressive act outside the uterus (that of grasping for air, reaching out for food and for contact), and all the way to mature sexuality, aggression is a self-assertive force, directed at being and at obtaining what is needed. It prompts behaviors that bring with them pleasure in movement, and in the exploration of the world. “This inherent, biological force should be allowed to be experienced fully as part of the individual’s journey towards individuation, creativity and being of realness.” (Ere’el, O. in Winnicott, D. W., 2009, p. 94).
Winnicott sees the whole spectrum of aggression as part of the early expression of love, “ruthless love”, in what he calls the “pre-concern” phase, when the baby is not aware yet of the results of his careless pushing and pulling, mostly of his mother’s face and body (ibid., p. 96). Later in development, aggression, in the service of forming a separate self, serves as the tool for establishing the distinction between what is “me” and “not me”. According to Winnicott, this process can happen when the small infant is allowed to express angry, rageful and even destructive impulses at the parent, who in return can survive the expression of those feelings, and not retaliate (Winnicott, D. W., 1971, p. 89–90).
When the parent can survive those expressions while creating a safe, containing environment for the infant’s expression, both the infant and the parent become more real, more separated, and actually are able to connect more fully. I’ll always remember a scene from when my son was two years old, verbal as ever, being very angry with me for I don’t remember what reason. He stood in front of me, shaking his two little fists at me and screamed, his face is fully red: “I hope a truck will run over you!” Then he took a breath, and kept looking for another horrible fate, “And – and a mosquito will bite you!!!” … Not too often in my maternal history did I feel pleasure like I did seeing the very alive body of my son, expressing an emotion I myself have never dared to express!
Failure to provide a safe container for the child’s aggression and negativity results in the requirement to hide those expressions. The degree and nature of the hiding, (using the child’s own biology and deformations as part of their character structure), vary. But in one way or another, the infant will always end up with bad feelings, and with various degrees of self-hate system like shame and guilt. Since the feeling is not met with some acceptance by the significant figures of that environment, it grows in one way or another, in the shelter of one’s being, to the point of perceiving oneself as evil, carrying feelings of sadism, violence and even perversion. Winnicott claims that when that happens, the person will separate good from bad, splitting to idealize objects on one hand, and create all-bad objects on the other. This splitting eases those difficult feelings so the splitting serves as a defense. (Winnicott, D. W. 2009, p. 97).
We can thus say that aggression, separated from the positive energy in it, becomes destructive, and can go so far that the person becomes hateful. This can be seen as a more developmental and dynamic explanation of Reich’s formulation mentioned earlier (Reich, W., 1942, p. 156), of how destruction and hate are formed by aggression that is emptied of love as a result of the child needing to split between those two components; or as how Lowen later phrased it as “hatred (that) can be understood as frozen love”. (Lowen, A. 1995, p. 172.)
The developmental processes involved in developing an entirely separate identity continue from about six months of age until about two and a half, or even longer. When a baby starts at about six months to push its mother’s body with its limbs, at the beginning of what Margaret Mahler called the separation-individuation phase, it is a beginning of the need to perceive the mother clearly from some distance, as well as turning one’s attention more outward. (Mahler). That process develops into the growing discrimination of “this is me – this is not me”, through movements of increasing force and intensity, like pushing, throwing, and biting as well as using his voice with a newer pushing quality and using the developing language to protest. Behavior becomes more and more purposeful and so does aggression. The organism gradually defines himself, his selfhood, in relation to his significant others to form his growing sense of boundaries. At this stage aggression helps make separation from others and create individuation. Healthy aggression is also self assertion, fueling the ability to say, “yes – this is me, this is what I want. Exactly this!” This is also a way of establishing differentiation, “I am me – I am not you, I have a mind and body of my own.” Still, those of us who raised children know what a child looks and sounds like when practicing exactly those capacities, wanting and not wanting the same thing at almost the same time. How unbearable it can feel and how patient a parent needs to be at times!
Yona Shahar-Levi, an Israeli senior psychoanalytically oriented movement therapist, in her book A body-movement –mind paradigm sees in the forceful, ballistic kind of movement, which is typical of that phase, as the engine of the process of separation and individuation. Its main task is recruitment of power, recruitment to get out of the body’s boundaries. It is the raw material of the potential of the vitality of the self. It stimulates the body to deal with gravity, to enlarge the personal space, and to gain a clearer perception of boundary between self and others.
Expression of opposition is crucial for feelings of identity, and for formation of true selfhood. The ability to say “no”, assert one’s self and set a boundary in response to environmental impingements is a very significant aspect in the functional – developmental role of aggression, in the changing ways it is manifested from conception to adulthood (Lowen,1970, p. 155).
In his book Pleasure, Lowen makes a correlation between the ability to assert oneself, to push away from oneself an undesired obstacle, to say “no”, to the quality of the protective boundary – the skin, the underlying fatty and connective tissue, and the striated or voluntary muscles.
“The limiting membrane, especially the skin, serves a protective function with regard to incoming forces. It allows the individual to screen stimuli and distinguish those that necessitate a response from those that can be ignored. When the skin is undercharged … the individual is easily overwhelmed by the stimuli which proceed from his environment … The ‘no’ functions as a psychological membrane that parallels in many ways the physiological membrane … It prevents the individual from being overwhelmed by outside pressures and allows him to discriminate among the demands and inducements to which he is constantly subject.” (ibid., p. 154–155).
Lowen also connects the ability to know oneself, to self assertion, connecting “no-ing” to “knowing”:
“The ability to negate, to put a boundary, is an ingredient of knowledge, and an important ingredient in forming a solid sense of self. Knowledge is a function of discrimination. Desires and impulses can only be known when they reach the surface or limiting membrane of the organism. The strength of the membrane depends on the inner charge of the organism … The right to say ‘no’ ensures the right to know … Simply stated, self awareness depends on self assertion. Asserting oneself implies the idea of opposition”. (ibid., p. 147–152).
So we can say that the availability for a human organism to grow into a person that allow aggression to go through its body is crucial for its liveliness, for its creativity and for the ability to serve as a safe, grounding container for oneself. Aggression allows for the ability to be an authentic, assertive, self respectful integrated self, for the ability to move towards another human being, and to form an intimate, sexual loving relationship.
Relational Conditions Affecting Development of Aggression
The capacity of a mother to supply an alive, attuned, pulsating physical and emotional ground onto which her developing infant can fully let go in the ever-changing ways he needs to, and from which he can find his spontaneous gestures, is one of the most significant ingredients for the development of a contactful, self-respecting, healthy human being, and for the development of healthy aggression.
A crucial element for good-enough parenting, is the ability of the parent to lend aspects of his/herself for the use of the child, and to be for him what Kohut calls a “selfobject” figure (Kohut, H. 1984, p. 49–50). Some of the most significant aspects of this function are those of empathy, of mirroring, at times of adoration, and of the enabling of the parent to let the infant immerse, and deposit in her/him the difficult, painful, unbearable feelings, including those of hostility and hate. This, and the ability of the parent to own and correct empathic failures, is the main vehicle through which this process can take place, so that the infant’s experiences can be digested, and especially that the unbearable experiences can transform into more bearable ones. Serving as a selfobject for the infant requires, in inter-subjective terms, “suspension of the parent’s subjectivity”, (Sara Goldstein, psychoanalyst, 2011, private lecture). This ability is especially significant and not always easy when it comes to responding to aggressive expressions, especially the ones that are more forceful, or that express opposition to the caretaker.
Alice Miller, in her book Prisoners of Childhood (aka The Drama of the Gifted Child) says: “Every child has a legitimate need to be seen, understood, attended to and respected as he is, with his feelings, sensations and expressions” (Miller, A. (1979), 2000, p. 24). Only with that quality can he ground in his mother’s eyes and body. However, “parents can give their child the atmosphere of healthy development only if they grew up in such an atmosphere … If not, they will often look for a person who will give himself to them fully, be fully attuned, understanding, etc. The most immediate figure to fulfill that role is the person’s own child” (ibid., p. 24–25). In such cases the parent often looks at the child, thinking: “Don’t be who you are, be who I need you to be; who you are disappoints, threatens, angers and over stimulates me. Be what I want and I will love you” (Johnson, S. 1987, p. 39). In response the child, not seeing in the parent’s eyes the reflection and mirroring that are crucial for healthy development, but needing the vital connection more than anything else for his survival, starts giving up his authentic self-expression, identifies with his parent’s expectations of him and sponges through his eyes, skin, nervous system and his whole being the energetic qualities he senses from the parents. He becomes the container for his parent’s depression, anxiety, horror and misery, taking in the energy directed at him. Instead of an authentic free self-expression, the child minimizes his motility, his breathing, and thus his liveliness. In this condition, any expression of aggression, of moving from within, of anger, of protest and mostly of separateness – is impossible. It goes against his forced existential task – to be there for his caretaker.
In such dynamics the aggressive movement will come out in distorted, contactless ways – he will develop, as noted before, different kinds of self hate systems, like guilt and shame, turned against the self, and/or, it will come out in rage, destruction, hate, violence, sadism, and/or abuse. It is crucial to emphasize that what enables this dynamic is the existential dependency of a child on his parents, and the fear of losing it. The unconscious demands parents put on their children to be attuned to their needs, to fill the void in them, to be the way they expect them to be, along with the intolerance they manifest toward the child’s spontaneous gestures of vitality, or the way in which he moves out to the world, is what is perceived by the infant as a threat of rejection, of withholding of parental love. This dynamic can actually be found, in some way or another, in the core of any character formation.
The etiology of this kind of relational abuse in families is widely varied. It often involves traumas of different kinds that the parents went through. If the anxiety of the trauma is not processed by the parent, it will be inserted into the child’s body, which in return will look for comfort, with the price of giving up a big part of his authentic needs. The child’s excessive dependency and the parent’s damaged integration will form a ground for the parent using the child for her or his own needs, and for the interruption both in healthy developmental processes and in the formation of healthy aggression.
From my own personal experience, and from that of many of my patients, I believe that in families where there is a history of exposure to trauma involving threat of death, or in areas where existential issues are not just a philosophical question, the fear that enables this dynamic is not just that of abandonment, but rather that of actual annihilation. In those families the basic knowledge that life is an ongoing process is not obvious, and that heightens the anxiety and subsequently increases the dependency.
That phenomena, i. e. that an environment producing fear and anxiety will affect the possibility of people to have their healthy aggression is supported by Lowen from his basic energetic point of view, stating that aggression and fear are antithetical in the way they flow in our body, and cannot exist together – aggression flows from the center up and down to the extremities of the body, while fear flows from the extremities towards the center. (Lowen, A. 1995, P.105.)
Clinical Cases in Working with Aggression in Bioenergetic Analysis
In this part of the paper I would like to demonstrate through clinical material how I work with aggression, keeping in mind the history and development of patients and their character structure. I will use parts from sessions with two of my patients. Then I will shed light on some issues that I find significant while working with aggression.
The Case of M.
At the very core of healthy aggression is the movement of extending oneself, reaching out for contact with the world and for the satisfaction of one’s needs. The ability to do this is the essence of initiation. As I discussed earlier, when the individual has to be fully attuned and reactive to his environment for his survival, the spontaneity of any authentic movement is frozen by a chronic fear, and his aggression is blocked, at times – like in the case I want to present – very profoundly.
M. was a male patient in his late fifties, who immigrated to Israel from Holland in his early twenties with his family. Both his parents were Holocaust survivors. His father, who was sixteen when the Nazis invaded Holland, was separated abruptly from his parents, being taken together with other Jewish children to England, leaving the rest of his family behind forever. They were later killed in Auschwitz.
In the early 1950’s the father married a Jewish German woman and they had three children. M. is the middle child. The father, who worked as a traveling salesman was very depressed, and did not have much contact with his family members. He used to sleep with his passport under his pillow, “just in case”. There was always a feeling of transience at home.
The mother was an extremely impulsive, intrusive, manipulative and very emotionally unstable woman. With the emotional absence of her husband and her older son being quite problematic, most of her needs were directed at M., who, as a little boy, had no option but to be fully attuned to her and her mood swings. He often described her as trying to “swallow” and merge with him. He was fearful of suicidal threats she would often express and of her hysterical, quite violent, at times very sexually provocative attacks. The combination of shock, horror and some sexual excitement he would often experience around her and the general atmosphere at home affected him deeply. He was never able to let down into his own body, or feel safe on this unstable, horrifying, over-stimulating ground.
M. is a pleasant looking man with some schizoid traits – his body structure looks a bit disproportionate, body parts seem to be glued together. He often reports feeling a band of tension around his head, as if holding himself in the world through his thinking, fearing he will be annihilated if he lets go of it. He has a small belly, with a line of tension right above his genitals.
In his early life he developed into a lonely, quite depressed, unlively, fearful, insecure, mostly detached man. Closeness with another human body is experienced as a threat of invasion, of being used and swallowed-up by the other person, and of feeling shamed and humiliated when his emptiness and neediness is exposed. He lives alone and never has had a meaningful intimate or sexual relationship. Even though he holds a respected professional position, contact is often perceived by him as dangerous, like quicksand. This can explain the tentative contact he makes with the ground while walking. The option of a longitudinal energetic streaming connecting his heart to his genitals seems to be impossible. He often reports feeling chills in his gut. Even though he is very reluctant to do any kind of bodywork between sessions, even short walks, he responds positively to working with his body in our sessions, often initiating and directing it toward what he wants.
In the session I want to describe, we talked about his loneliness, his difficulty to initiate or even respond to social plans, feeling that in every relationship the other person’s needs takes over his; that in anticipation of any interpersonal contact he always predicts feeling used, even though very often he ends up having a good time. “It is as if the fear that I’ll be invaded erases the memory of the good feeling and so I don’t initiate social contact …” I suggested that if he wants, we could try to explore that fear. We got up, and he grounded himself, like he usually does, for a few minutes.
When he rolled up to a standing position his eyes were closed. I asked him what he sensed in his body. He said that he could feel some streaming in his legs, arms and genitals and the sensation of a slight expansion in his belly. We were facing each other. I noted that his eyes were closed. In response he opened them, and we made some eye contact. A second later he said: “Now the feeling of expansion is gone. The moment I sense even the slightest movement from you – my belly contracts and I feel like there is a shield in the front part of my torso.” After another moment he said – “I can’t stay relaxed when I am facing you like this, while standing up”. I ask if he wants to explore if there is any way he can organize himself, so that he doesn’t have to tense his body in my presence. He chose to lean on the wall, then asked to put a big ball I have in my office behind his back. I suggested that he let himself feel it, and the support from the floor under his feet. After a minute or two he said he could let go a bit of the tension in his belly. I stood in front of him, feeling more relaxed in my own body, thinking of how I can help him gain some control over whether he feels invaded or not, while feeling that he has some boundary, so that he has more freedom to initiate contact.
I suggested that he try lifting his arms forward very slowly and flex his palms facing towards me, kind of like a “stop” gesture. He didn’t even manage to get his arms all the way up, when he stopped. “No. It feels too scary … Now my belly is cold” he said, and dropped his arms. When I asked what he was afraid of, he answered: “I can’t trust that it is okay for me to set any boundary, and that you will not react.” When we talked about what reaction he feared, he could see clearly that for him, having contact brings up a fear of being invaded by a “wave of chaos” and that setting a boundary can evoke rageful retaliation by the other. Both options freeze him up. He connected the chaos to a recurring experience of his mother responding to any expression of feeling that was initiated by him, (especially if he dared to want something) with either her rage, to the point of slamming doors, or with being too intrusive, including with seduction, with no respect for his boundaries. This would make him feel annihilated, like there was no room for his own feelings, needs, and probably his own separate existence in the face of hers. Still, doing anything active to defend against it was impossible.
After a few minutes of talking about his experience, he said that he did not have any recollection of ever feeling like he could just “let go, rest”, unless he was fully alone. I connected this to his difficulty of being with himself in the presence of another, knowing that he could never have such an experience in the presence of his mother. I suggested that he lie down, try to feel the support of the mattress underneath him, and invited him to breathe. His breathing was very shallow, and I could sense some heaviness in my own chest. After a few minutes of doing just that, he realized that the actual act of inhaling, of taking in the air, is difficult for him. I realized that for M. the very core of aggressive movement, that of initiation of any movement out, including reaching out for air is quite frozen. I was becoming aware that to help mobilize his aggression, we should work on mobilizing his breathing. I suggested that he focus on breathing out with some force; try to push the air out, thinking that this can increase the volume of the whole spectrum of his breathing, and also incorporate some force into it. After a minute or two I suggested that he try to add some sound to the breathing out. Making sound is always difficult for him, so I found myself breathing out with him, and making some sound myself, which was helpful to him, to the point that he was able to breathe out with a louder voice, and pushing the air out with more force. After a few minutes he stopped to rest. His whole breathing, including breathing in (reaching out for air), was much fuller.
With the development of our work, a very moving process started taking place. I will not describe it in length, but just say that in the context of helping a patient find and expand the roots of his aggression, I constantly keep in mind that this force starts with the capacity to come out with one’s needs and wishes. We started taking the time, looking and listening very carefully, following as much as possible his movement, researching what he feels in his body, and what he needs and wants at any given moment. As part of this process I used two flat containers made of soft plastic wrapped with cloth that can be filled with warm water (what we call “hot bottles”) in response to his direct request to feel soft, warm bedding under his back and pelvis and on his chest. As our work progressed he became aware that in order to fall asleep he began to push his feet into the edge of the bed with some force. This brought up in me the associations of both an embryo pushing into the wall of the uterus (he often describes desirable sensations that sound like those of a fetus), or of a baby pushing his mother’s belly as a way to start separating from her. For someone like M., who had to be so reactive to his environment, accompanying him on this ongoing journey in finding, literally, his own movement, has been a very moving process.
The Case of D.
We can say that when a person does not have the freedom to set any physical and emotional boundary in relation to his significant others, or to express any opposition – it can affect the formation of physical selfhood, of his limiting membrane, and of serving as a container for himself. Encouraging expression of negativity, anger, rage etc., together with reinforcing a sense of boundaries, is very helpful, like in the case of D.
D. is in her late forties, short, blond and blue-eyed. What characterizes her body structure is that it has no clear structure, a bit formless. When first meeting her I found myself wondering how much is this woman allowed to be, to have a form. Her legs are not weak, a bit stocky, somewhat masochistic, but she seems to not use them fully as her base of support. Her outer pipe, mostly around her pelvis and torso, feels unformed, weak, not toned, not alive and not integrated with the rest of her body. She leans forward, as if looking for support. When she looked at me for the first time, it was as if she wanted to go inside me and make there a home for herself. That fits in many ways with the way she tends to be in the world, constantly looking for reassurance from the outside.
This can be explained by elements in her history. She is the second daughter of a father who is a very successful, famous professor in the University, and a mother who was a teacher. Her father was originally from Poland, suffered severe traumas as a child in the WW2 and later was badly injured in the war of 1948. Being as emotionally injured as he was, the father became bitter, offensive and heartless. His main interaction with his children has always been wanting them to hear his horror stories. Her mother, a very beautiful and very depressed woman, stopped working and spent most of the time in bed with tranquillizers. She never loved her husband. My patient, from a very young age, stayed home with her mother making sure her mother was okay. She slept in her parent’s bed on and off until she was an adolescent, as a way to soothe her mother’s fear, and probably protect her from what the mother experienced as her husband’s repulsive sexual demands. Any movement towards separation would be met with blaming her for lack of empathy. D’s only comfort was food, and she developed a severe eating disorder. In her mid-twenties she finally left home and even moved to another country for a few years, as the only way she could detach herself from her parents.
D. is weak, depressed and very anxious. She is married and has two children, is intolerant to their imperfections, and often explodes in raging attacks at them. The role of her husband in the first years of our therapy was to serve as the container for her bitterness and rage, and also to save her when she felt panicked, which would happen often. That was also a lot of what she needed me for, every time arriving with handful of problems. It became clear that letting down into my holding, that at times included physical holding, was not always easy or couldn’t fill her emptiness for more than a few hours. Often she would question my ability to help her, always with a flavor of suspiciousness and negativity. It took a few years before she could be more direct with her negativity and a few more before she could let herself open her heart to me more fully.
Despite her poor relationship with her body, she began to use body work very extensively, working a lot with breathing, grounding, expressing and discharging feelings of rage and deep pain, with a growing capacity to do it with me, not next to me, and with a growing ability for me to deeply feel for her. With the help of our work and couples therapy she had with her husband, her relationship with her husband has changed, so that he treats her much more as an equal.
I want to present part of a session I had with D. She arrives upset after a visit she had to her parent’s house, who are now over eighty.
“I can’t stand my father. He is unbearable. He complains about feeling depressed, and my brother and I are doing nothing for him. I try to tell him that he should get psychiatric help. He says that no one can help him besides us because he is a ‘special case’ with all the things that he went through. He is so demanding and entitled!! All he wants from us is to listen to his sufferings, and to his horror stories. To spill his shit onto us. He even complains that Mica (her five year old daughter) doesn’t care about how he feels …” (She sounds more and more in despair and enraged.) “He is crazy! I won’t let him do to my kids what he did to me!”
She starts crying, but her crying is not fluid. It is choked. I also notice that her legs are moving restlessly as she is talking. I invite her to focus on her body, and feel if there is any impulse that needs to come out. She says she wants to kick, moves to the mattress and lies down. I sit next to her, suggest that she lift her legs with flexed feet towards the ceiling and stay there for a while, thinking that this way her pelvis is supported while she grounds and charges her legs towards the kicking she expressed the need to do. After a few minutes she starts kicking with a sound, a mixture of crying and some rage, but her throat still seems a bit choked. It feels like her charge is condensed with a mixture of anger, rage and also despair.
While resting, I suggest that she focus on her breathing and try to breathe out more fully. After a short while she starts crying again, deeper. “He still has such an effect on me! Both of them, you know … like an obsession … It’s so difficult to be there and let him just feel bad. I feel so guilty … I also think that I am still scared of him”. She keeps crying, “This guilt is like jail! I want to get out of his jail!” As she is saying it, she starts moving her legs with growing force, kicking, screaming, and crying, “Leave me alone!” while banging both fists on the mattress. I pay attention to my breathing, making sure I am present with myself. After a few minutes she calms down. We are in a more relaxed quiet contact. “Do you know why you are afraid of him?”
“I forget that he is a weak old man now. For me he is still this controlling, scary, strong, demanding man, this famous person that every one admires, that I have to comply with; I can still feel so easily humiliated by him … Tomorrow I am going to meet them. I want to be able to not be so affected by him! To not feel helpless in his presence and lose myself …”
I ask her if she would like to do some related bodywork to prepare for their meeting. She agrees. I suggest she stand, feel herself and feel the space around her body. Take the time to do so. See if she can try to feel it as hers, that no one can go in without her permission. It’s difficult for her. I suggest she widen the stance of her feet. Try to feel her center like an inner pipe; try to contract this “pipe” a bit, as to get a clearer feel of having a center in herself that she can rely on. Then I ask her to gradually bend her knees and arms, and start pushing from the center. I invited her to see if she wants to also push with her voice. She started very slowly, and as she kept doing it she put into her pushing more and more strength and used a louder voice. It looked as if she enjoyed it. When it was time to stop, she had changed. She looked at me, smiling, “He is just an old man, after all …”. I could even trace a seed of compassion she could allow herself to feel for him now.
Three Aspects of Working with Aggression in Bioenergetic Therapy
I want to briefly review some of the significant aspects of working with aggression in Bioenergetic therapy:
1. Character Analysis
Deep analysis of how aggression from the start was met by the significant environment, and how this encounter affected this force – where could it continue with its flow, how was it stopped, or what kind of by-passes did it have to take in response? This analysis should take place on all levels – physical, emotional, mental and behavioral. A significant part of this work should take place in the context of the therapeutic relationship.
2. Physical – Energetic Work
Outside of the limbs, the main muscle mass of the body associated with aggression is located along the backbone. The flow of energy goes upward along the back and into the head, the eyes, mouth, teeth, throat and arms and leads to aggressive activities in the upper half of the body – breathing, looking, sucking, biting, reaching out, pushing, hitting, squeezing and vocalizing. When energy or feeling flows downward into the pelvis and legs, it leads to aggressive actions with the lower part of the body, some of which have to do with discharge: kicking, pushing out the body’s excretions, and sexual activities (Lowen, A. 2005, p. 302). In order for aggression to move freely, the outer and inner tube of the body should be relatively free of tensions.
Since breathing was the first aggressive movement in each of our lives and aggression always needs a ground to lean on it is important to remember that opening breathing and deepening one’s grounding are always necessary when working with aggression. It is also important to remember that working with sexual issues is a significant aspect of working with aggression. Helping a patient find his own movement and integrating the work gradually can be crucial for a cohesive healing process, moving them towards an authentic self-motivated being.
3. Relational Aspect in Working with Aggression
From the very basic element of the aggressive movement, that of reaching out, through the expression of assertion and anger, and even more so – in dealing with the more negative range of aggressive feelings, like rage, hate, and violence – it is important to remember that those gestures are always relational. Those expressions were stopped in childhood, having to change their path, because of some negative, inappropriate response from the significant figures, either actual or internalized, such as parental contraction, withdrawal of love, disrespect, humiliation, revenge, hostility, hate, and the like.
Encountering the monstrous, rageful feelings in oneself is one of the most difficult and unbearable aspects of the therapeutic journey. I know it from my own process and from working with patients. It is important to emphasize how it is crucial that the therapist treats this zone with much compassion, empathy and respect, helping the patient understand its origins. When the therapist, because of their own vulnerabilities, responds with condemning, sadistic or humiliating responses, the abusive or hurtful historical dynamic is being reenacted, and will deter the patient from expressing such feelings in the future.
Still, receiving the expression of aggressive negativity can be very difficult for a therapist, especially when those expressions are directed, usually as part of the transferencial aspect of the relationship, toward the therapist. This is where the depth of professional integrity, together with the capacity to recognize and contain countertransferencial reactions, like one’s own anxiety, vulnerability, and unworked through narcissistic rage, are being tested. When saying that, I do not mean that we should never set a boundary, when we feel that we were abused, but not before checking thoroughly if we are responding to our own historical dynamic. I also don’t exclude, when it is appropriate, sharing with the patient how we are made to feel. But it should always be accompanied with expressing an empathic understanding of the patient’s dynamic.
It is not an easy task. One of my patients, fitting the description of borderline-narcissistic structure, is so sensitive to any empathic failure, craving for a perfect attunement, that I encounter his narcissistic rage directed at me in almost every session. I often feel that my main task is to survive it – To just keep breathing. I can sense in myself how I freeze, at times dissociate, feeling deep fear, and in some moments I find myself hoping he just gets up and leaves.
Winnicott, in his article – The Use of the Object and Relating through Identification takes the relational aspect in working with aggression one step further. He claims that in the same way he perceives the caretaker surviving expressions of anger and rage as a condition for healthy developmental changes in the child to take place, a necessary condition for real change in the therapeutic process to genuinely take place is for the therapist to allow the patient to get angry, even enraged at him, and for the therapist to survive it. He says: “(Real changes) … do not depend on interpretative work. They depend on the analyst’s survival of the attacks, which involves and includes the idea of the absence of a quality change to retaliation.” (Winnicott, D. W., 1971, p. 91)
Margit Komeda-Lutz, in her article Is there Healing Power in Rage when discussing the healing aspects of freeing the expression of anger and rage, emphasizes the significance of careful attunement to the strength of the therapeutic bond, at least for certain kind of patients, when working with such expressions. “For weakly structured patients, and at least at the beginning of treatment, such techniques (designed for strong discharge), are less indicated. These patients first needs are to establish some reliable bond to a trustworthy person, they must build ‘psychic containers’ big enough to tolerate and cope with intense emotions”. (Komeda-Lutz, M. 2006, p. 121)
Summary
Aggression is one of the most significant forces supporting the basic elements of healthy development, starting from breathing, initiating contact with the outside, asserting one’s needs, protecting its integrity through setting boundaries and using anger to push whatever is threatening away. Aggression is also the force that supports healthy separateness on one hand, and intimate relatedness on the other.
An environment that supplies an alive and attuned ground with the parent (and later the therapist) lending needed aspects of himself into which the developing infant can fully let go, is crucial for the development of healthy aggression. When the parent, because of her or his own history, instead of being there to fulfill a child’s emotional and physical needs, uses and exploits the child to fill the void in her or him – the child will stop his spontaneous movement and will adapt himself in one way or another to what he senses that he is expected to be for the safety of his bond with the parent. Under such conditions healthy aggression cannot flow in the body, since it goes against its forced destination. Instead, the aggressive charge turns against the self in a variety of self-hate systems, and also is accumulated in one’s body, turning into rage, hate, and violence, which are all destructive forces.
Working with aggression in therapy, especially with the negative part of the spectrum, is not an easy task for any of us, and it often reactivates our own historical traumas around those exact issues. Still, since our patient’s healthy aggression, (like our own) was distorted because it lacked the needed relational components, it is crucial for therapy with those issues to be effective. In addition to the body-energetic work, we must position ourselves with the needed empathy and compassion towards our patient’s expression.
Footnote
- [1]
- Similar to Lowen’s perception of aggression, Winnicott opens this article, written in 1950, a few years after the discovery of the horrible results of the 2nd W. W. with an extremely important, still, unfortunately, very relevant statement: “The main idea behind this study of aggression is that if society is in danger, it is not because of man’s aggressiveness but because of the repression of personal aggressiveness in individuals.” (Winnicott, D. W. 1982, p. 204 emphasis added.).
References
Eigen, Michael (1999): Toxic Nourishment. Karnac, London.
Helfaer, Phillip (1998): Sex and Self-Respect. Praeger Publishers, Westport, CT.
Hilton, Robert (2007): Relational Somatic Psychotherapy. Bioenergetic Press.
Johnson, Stephen (1987): Humanizing the Narcissistic Style. Norton & Company, N. Y.
Kohut, Heinz (1984): How Does Analysis Cure? The University of Chicago Press, Chicago.
Komeda-Lutz, Margit (2006): Is there Healing Power in Rage?-The Relative Contribution of Cognition, Affect and Movement to Psychotherapeutic Processes. The Clinical Journal of the IIBA. Vol. 16, p. 103–127.
Lowen, Alexander (1975): Bioenergetics. Penguin Books, N. Y.
Lowen, Alexander (1995): Joy. Arkana – Penguin Books, N. Y.
Lowen, Alexander (1958): The Language of the Body. Macmillan Publishing Co. Inc. N. Y.
Lowen, Alexander (1970): Pleasure. Arkana – Penguin Books. N. Y.
Lowen, Alexander (1983): Narcissism: Denial of the True Self. Macmillan Publishing Co. Inc. N. Y.
Lowen, Alexander (2005): Aggression and Violence in the Individual. In: The Voice of the Body – The Role of the Body in Psychotherapy. Selected Public Lectures, 1962–1982. Bioenergetic Press.
Mahler, Margaret. Pine & Bergman, (1975): The Psychological Birth of the Human Infant. Karnack Books, Great Britain.
Miller, Alice (1979): Das Drama Des Begabten Kindes, und die Suche nach dem wahren Selbst. Hebrew translation (2000), Dvir Publishing House, Tel Aviv.
Reich, Wilhelm (1972): Character Analysis. Touch Stone, N. Y.
Reich, Wilhelm (1973): The Function of the Orgasm. Farrar, Straus and Giroux. N. Y.
Rizzuto, Ana-Maria, Meissner, W. W., Buie, Dan (2004): The Dynamics of Human Aggression. Taylor & Francis Books, N. Y.
Shahar-Levy, Yona (2004): A Body-Movement-Mind Paradigm. Jerusalem, Israel.
Winnicott, D. W. (1971): Playing and Reality. Tavistock Publications, London & New York.
Winnicott, D. W. (1950–1955): Aggression in Relation to Emotional Development, in: True Self – False Self – collected Essays – Hebrew Translation (2009). Am-Oved, Tel-Aviv.
Abstracts
German
In diesem Artikel wird Aggression in einem weit gefassten Sinne untersucht, und zwar aus der Perspektive psychoanalytischer Literatur mit einem Fokus auf Bioenergetische Theorie und Praxis. Die Untersuchung der Arbeit mit der Aggression von Patienten wird mit klinischem Material angereichert, einschließlich der energetischen Arbeit mit Atmung, Erdung, Grenzziehung und von Ausdrucksbewegungen. Aus der Perspektive einer relationalen Matrix und im Zusammenhang mit Fragen der Gegenübertragung untersucht dieses Papier den Umgang mit Aggression in der therapeutischen Arbeit mit schwächer strukturierten Klienten.
French
L’agressivité est regardée, dans le sens large du terme, du point de vue de la littérature psychanalytique, se concentrant sur la théorie et les interventions du point de vue bioénergétique. Le matériel clinique met en valeur l’exploration du travail fait sur l’agressivité exprimée par les patients, comprenant la dimension énergétique produite par les interventions faites sur la respiration, l’enracinement, la mise en place des frontières et les mouvements expressifs. Ce texte étudie également comment utiliser le travail sur l’agressivité lorsque nous travaillons auprès des structures de personnalités fragiles, comme intervenir dans la configuration relationnelle et lorsque nous rencontrons des enjeux contre transférentiels.
Italian
Viene esaminata l’aggressività, nel senso ampio del termine, a partire dalla letteratura psicoanalitica con particolare attenzione alla teoria e al trattamento bioenergetico. Il materiale clinico potenzia l’esplorazione del lavoro con l’aggressività dei pazienti, compreso il lavoro energetico con il respiro, il grounding, la costruzione dei confini e i movimenti espressivi. Questo articolo esplora il lavoro con l’aggressività nelle strutture più deboli a partire dalla matrice relazionale e quando si incontrano problemi di controtransfert.
Portuguese
Neste artigo, examina-se a agressividade, no sentido mais amplo, a partir da literatura psicanalítica, com foco na teoria e prática da Bioenergética. O material clínico ajuda na exploração do trabalho com a agressividade em pacientes, incluindo exercícios energéticos de respiração, grounding, estabelecimento de limites e movimentos expressivos. O artigo aborda, também, como lidar com a agressividade em estruturas frágeis, quando se trabalha a partir da matriz relacional e quando surgem questões contra-transferenciais.
Russian
Рассматривается агрессия, в широком смысле этого термина, как это принято в психоаналитической литературе, с акцентом на биоэнергетическую теорию и практику. Даются примеры терапевтической работы с агрессией у клиентов, включая энергетическую работу с дыханием, заземлением, установками для работы с границами и экспрессивными движениями. Рассматривается терапия агрессии у пациентов со слабыми структурами при работе в системе отношений, сопровождаемой проблемами контрпереноса.
About the Author
Anat Gihon, M. A. is a Movement Expressive therapist and a certified Bioenergetic Analyst living and practicing in Israel. She is a member of the IIBA faculty and head of the Training Committee for the Israeli Society for Bioenergetic Analysis, of which she was amongst its founders. Since 1987, Anat has had extensive experience in teaching the theory and practice of Bioenergetic Analysis in private workshops, academic programs for Movement Therapy and in the Training program of the ISBA. She is a graduate of the program for psychotherapy of the Israeli Institute for Psychoanalysis.
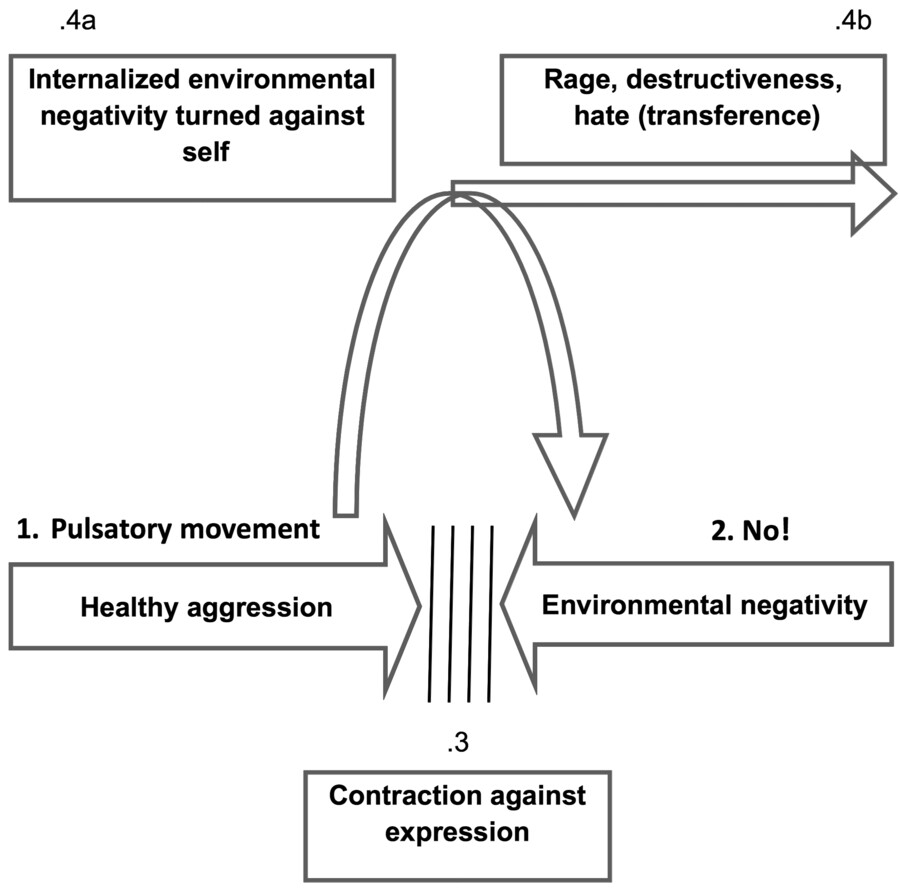
Appendix 1: The spectrum of aggression – based on R. Hilton’s formulation