Traumatic Memories
A Neuroscience Perspective
Homayoun Shahri
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2017 (27), 49–70
https://doi.org/10.30820/0743-4804-2017-27-49 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstracts
English
In this paper, a detailed description of formation of memory based on neuroscience is given. Different types of memories are reviewed, and definitions of repressed memories and dissociated memories are introduced. Formation of dissociated memories, as well as mechanisms of repression of memory, based on recent fMRI studies and neuroscience research, are discussed. It is argued that traumatic memories frequently have dissociated aspects and repressed aspects. It is concluded and shown, based on recent research in neuroscience, that regardless of the nature of traumatic memories, a very important factor in treatment of trauma is the attuned therapist and the therapeutic relationship. Finally, two case studies are presented to highlight the arguments set forth in this paper.
Key words: Amygdala, Hippocampus, Prefrontal Cortex, Traumatic memories, Neuroscience, Therapeutic Relationship, Attunement
German
Dieser Beitrag liefert eine detaillierte, neurowissenschaftlich fundierte Darstellung von Gedächtnisbildung. Unterschiedliche Gedächtnisarten werden referiert, und es werden Definitionen von verdrängten und von dissoziierten Erinnerungen eingeführt. Die Ausbildung von dissoziierten Erinnerungen und Mechanismen der Verdrängung von Erinnerungen werden mit neueren fMRI-Studien und neurowissenschaftlicher Forschung belegt. Es wird gezeigt, dass traumatische Erinnerungen häufig dissoziierte und verdrängte Aspekte beinhalten. Auf der Grundlage aktueller neurowissenschaftlicher Forschung wird dargelegt, dass unabhängig von der Art der traumatischen Erinnerungen, ein einfühlsamer Therapeut und die therapeutische Beziehung sehr wichtige Faktoren in der Trauma-Behandlung sind. Zum Schluss werden zwei Fallvignetten präsentiert, um die Darlegungen dieses Beitrags zu illustrieren.
Italian
In questo saggio viene descritto in modo dettagliato come si forma la memoria in base alle neuroscienze. Vengono rivisitati diversi tipi di memorie e vengono presentate le definizioni di ricordo rimosso e ricordo dissociato. Sono trattati la formazione dei ricordi dissociati e i meccanismi di repressione della memoria in base ai recenti studi fMRI e alla ricerca neuroscientifica. Si sostiene che i ricordi traumatici hanno frequentemente aspetti dissociati e aspetti repressi. Si conclude e dimostra, sulla base delle recenti ricerche neuroscientifiche, che, indipendentemente dalla natura dei ricordi traumatici, un fattore molto importante nel trattamento del trauma è la sintonizzazione del terapeuta e la relazione terapeutica. Infine, vengono presentati due casi clinici per evidenziare gli argomenti di cui al presente articolo.
Spanish
Este artículo ofrece una descripción detallada de la formación de la memoria basado en la neurociencia. Se repasan diferentes tipos de memorias y se introducen definiciones de recuerdos reprimidos y recuerdos disociados. Se plantea la formación de los recuerdos disociados y mecanismos de represión de la memoria basado en los recientes estudios de fMRI e investigación de la neurociencia. Así mismo se argumenta que los recuerdos traumáticos poseen con frecuencia aspectos disociados y reprimidos. Se concluye y se muestra en base a las investigaciones de la neurociencia, que independientemente de la naturaleza de los recuerdos traumáticos, un factor muy importante en el tratamiento del trauma es la sensibilidad del terapeuta y la relación terapéutica. Por último, se presentan dos casos con clientes para destacar los argumentos enunciados en este documento.
Portuguese
Este trabalho traz uma descrição detalhada da formação da memória, baseada na neurociência. Além disso, traz a revisão de diferentes tipos de memória, apresenta a definição de memórias reprimidas e dissociadas e discute sua formação e mecanismos, baseados em estudos recentes da fMRI e da neurociência. Demonstra, também, que memórias traumáticas têm, frequentemente, aspectos dissociados e reprimidos. Mostra, por fim, com base em pesquisas recentes da neurociência, que, apesar da natureza das memórias traumáticas, um importante fator no tratamento do trauma é a relação terapêutica – com um terapeuta sintonizado. Serão apresentados dois estudos de caso para demonstrar os argumentos aqui desenvolvidos.
Introduction
Trauma has a huge impact on all aspects of our society and civilization. However, the existence and reality of trauma is not considered to the extent that it should. The effects of trauma are rarely acknowledged and are often neglected. Trauma can alter the individual in his or her very core, and affects all aspects of life. Trauma changes the way an individual interacts with his or her environment, his or her flow of information, and flexibility of responses to their surroundings. Trauma may change the body of the individual, making it rigid at times or flaccid (collapsed) at other times, resulting in a loss of motility and limiting the individual’s aliveness. It may also change the functioning of the internal organs. Trauma may change an individual’s metabolism of energy, and exchange of energy with the environment. Traumatized individuals are prone to primitive self-protective responses when they perceive certain stimuli as a threat. Once sensory stimuli trigger past traumatic events, the emotional brain activates the old habitual protective responses resulting in an inability to self-regulate. At the core of understanding trauma and healing trauma, is the nature of traumatic memories and their activation. In this work, I shall look at traumatic memories in detail and bring together results from neuroscience and psychology.
Shock trauma is sudden, massive, and may be chronic. It affects individuals in their core, and may alter the functioning of the brain including the frontal cortex, limbic system, parietal lobe, insula cortex, and visual cortex, etc. (van der Kolk, 2014; LeDoux, 2002). This is in contrast to developmental trauma, which usually is chronic, happens during developmental stages, and is mostly due to non-optimality of caretakers responses to the developing child. Developmental trauma can and does affect brain functioning but generally not in the same way as shock trauma. Developmental trauma is also referred to as complex trauma (van der Kolk, n. d.).
Recently, healing of trauma, including PTSD, has found quite a lot of interest within the research community. This interest in studies of trauma, its causes, and healing is partially fueled by recognition of its existence, and to recent technological advances in neuroscience and brain imaging (notably fMRI), as well as a changing political climate. In the following section, I will discuss the nature of traumatic memories from the standpoint of classical psychology as well as recent advances in neuroscience.
Neuroscience of memory – a microscopic view
At the core of the brain are the neurons. There are about 100 billion neurons in our brain, and each neuron can have thousands of connections with other neurons. Neurons communicate via their axons (transmitters) and dendrites (receivers). A neuron can have thousands of dendrites, thus receiving input from thousands of other neurons. Neurons however, usually have one axon, but axons can have many branches as shown in Figure 1.
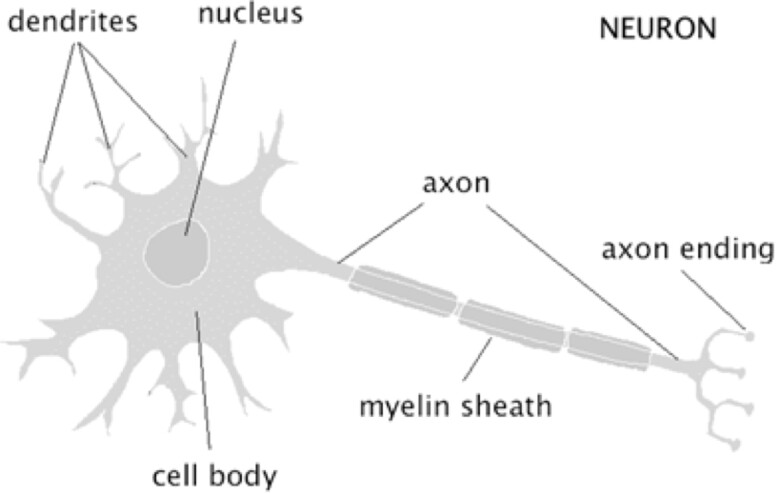
Structure of a neuron
The junction where an axon meets a dendrite is called a synapse. The neurons transmit information by their axon to other neurons through synaptic space. When an electrical signal reaches the end of the axon it releases neurotransmitters contained in Vesicles (see Figure 2). These neurotransmitters travel through the synaptic space and bind to dendrites of other neurons, resulting in electro-chemical changes in the body of receiving neurons. There are two general types of neurotransmitters, these are inhibitory and excitatory neurotransmitters. Excitatory neurotransmitters stimulate the brain (increase the potential buildup in the receiving neuron), while the inhibitory neurons calm the brain (reduce the probability of potential buildup in the receiving neuron).
The main inhibitory and excitatory neurotransmitters in the brain are Gaba (Gamma-Amino Butyric Acid), and Glutamate respectively. There are also other neurotransmitters that play a significant role in brain information processing and memory, which I will discuss below. When the receptors on the receiving dendrites bond with the neurotransmitters, and electro-chemical change inside the neuronal cell takes place, this results in increase of the internal potential of the neuron from a resting voltage of –70 mV to possibly a voltage of +40mV. At this point the charge rapidly decreases to –90 mV, which results in release of neurotransmitters into the synaptic space of the receiving neuron through its axon. This event is called action potential and the rise and fall of potential is called a spike, which is shown in Figure 3, below.
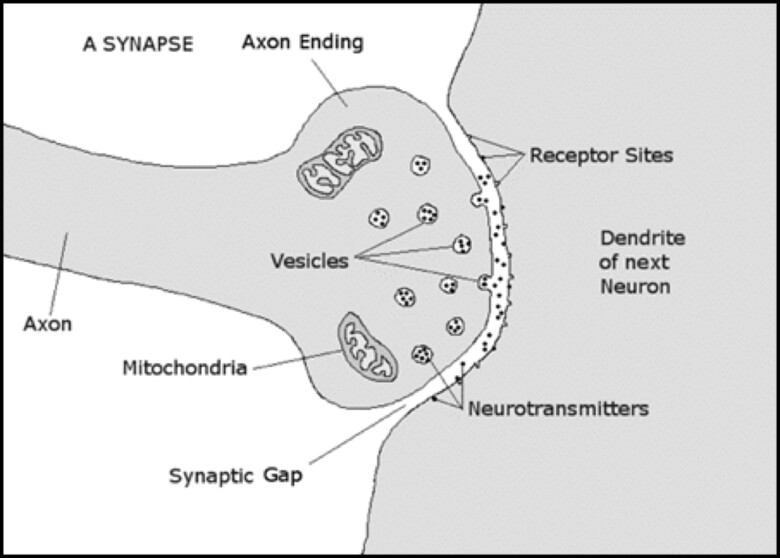
Structure of a Synapse
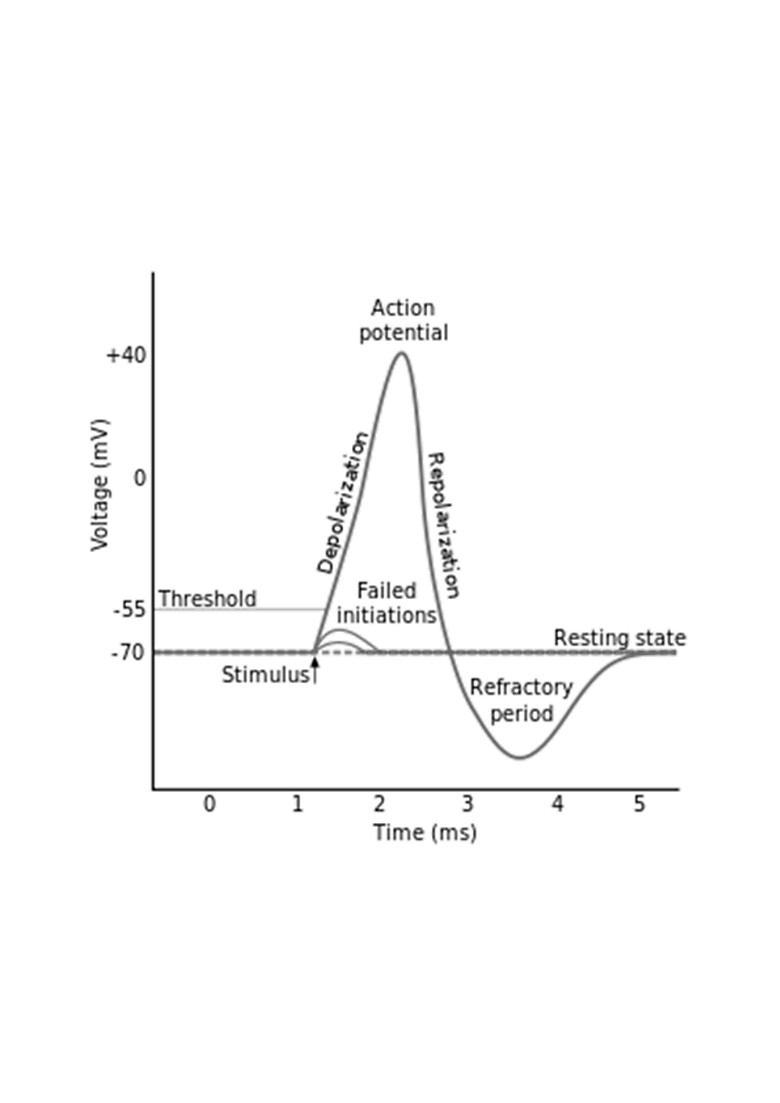
Formation of action potential (spike)
A neuron usually releases a sequence of spikes called a spike train, or a train of action potentials. Information is carried in the spike trains. In order to gain a deeper understanding of this process, please refer to Figure 4.
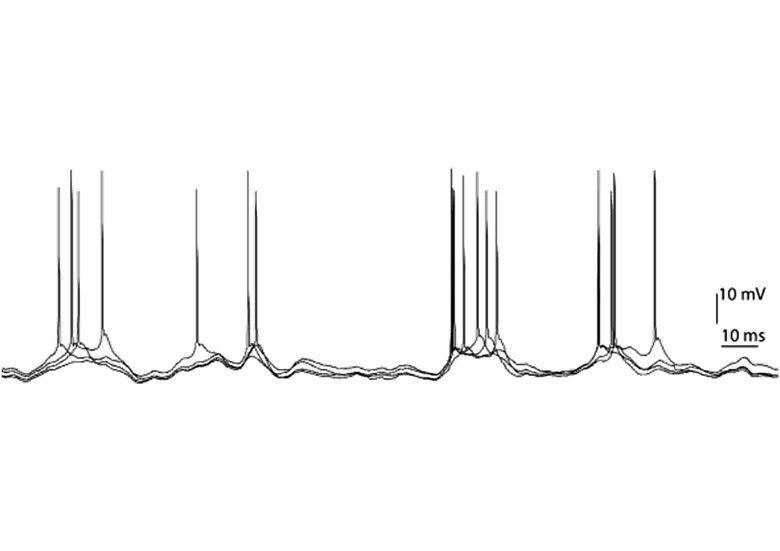
A spike (action potential) train
However, neurons do not function in isolation. The axon of one neuron may form synapses with dendrites of many other neurons. Of course many neurons may fire action potentials at the same time, thus the question is, what happens when many neurons are involved in generating action potentials. In other words, what is the mathematics of synapses? LeDoux (2002) indicates that the principles of synaptic mathematics are: Exuberance – that is more synapses are made than are preserved; Use – that is the synapses that are preserved are the ones that are active; and Subtraction – that the synaptic connections that are not used are destroyed. This clearly points to synaptic plasticity. That means the brain is constantly in the process of rewiring itself, thus forming new synapses, and destroying others.
Neural networks and memory are associative. Associative memory is defined as the ability to learn and remember the relationship between unrelated items. Let us now discuss the associativity in formation of memory in neural networks. In 1949, Donald Hebb suggested that if the axon of neuron A is close enough to the dendrite of neuron B to excite it and result in action potential, and if the process occurs repeatedly and consistently, then the connection between neurons A and B will be strengthened, and will result in higher likelihood that neuron B fires an action potential in response to neuron A. In other words, neurons that fire together wire together, and this is known as the Hebbian axiom, which also describes the essence of learning and memory (LeDoux, 2002). Much has been discovered about the underlying mechanism of Hebb’s fire-and-wire theory which involve sodium, potassium and calcium ion channels and NMDA receptors, which are special glutamate receptors that pass calcium resulting in long term potentiation (LTP – long lasting increase in transmission, which results in a longer spike train), when both the presynaptic neuron (through its axon) and postsynaptic neuron (through its dendrites) are active at the same time. LeDoux (2002) writes:
“Presynaptically released glutamate finds its way to both AMPA (a glutamate receptor involved in regular synaptic transmission) and NMDA receptors. Binding of glutamate to AMPA receptors is one of the major ways that a postsynaptic cell can be induced to fire an action potential, and is the means by which cells normally get fired up. In contrast, when presynaptically released glutamate reaches NMDA receptor on the postsynaptic cell, it has no effect initially because part of the receptor is blocked (by Magnesium – Mg). However, once glutamate has activated the post synaptic cell (caused it to fire an action potential) by binding to AMPA receptors, the block on the NMDA receptors is removed, and glutamate can open the receptor channel and allow calcium to enter the cell. LTP is the result.” (p. 144)
This is the essential requirement for Hebbian neural plasticity. LeDoux (2002) describes NMDA receptors as “coincidence detectors”, which detect the coactivity of both presynaptic and postsynaptic neurons, and more importantly according to LeDoux (2002) they detect which presynaptic neurons where active when the postsynaptic neuron fired an action potential. This is the essence of associativity of neural networks.
Hebb’s Theory Applied to Formation of Memory Based on Associativity
LeDoux (2002) writes:
“In order for two stimuli to be bound together in the mind, to become associated, the neural representations of the two events have to meet up in the brain. This means that there has to be some neuron (or a set of neurons) that receives information about both stimuli. Then and only then, can the stimuli be linked together and an association be formed between them.” (p. 135)
Many neuroscientists as well as psychologists believe that memories are represented by associative neural networks which are structures in which various aspects of memory are represented separately and also linked together (LeDoux, 1996). In order for the memory to form the associative network, it has to have reached a certain degree of activation, which is dependent on the constituent components of memory, as well as the weight of each component. The weight of the components is dependent on the cues that were present during the learning process, and are also present during recall. These cues in many cases are emotions associated with the components of memory. Thus as a given component of memory is activated due to presence of a given cue, the activation of the full associative network is also facilitated. The cues in this case may be signals from brain and the body (emotions) that indicate that we may be in the same emotional state as during the time of formation of memory (LeDoux 1996). At this time it is also very important to emphasize that memories are a reconstruction of events at the time of recall, and thus our emotional state can influence the way the recalled memory is remembered. And the converse is also true in that memories are recalled and remembered best when one is in the same situation or emotional state (LeDoux, 1996). In particular, not all aspects of an experience are remembered in the same way, and emotions may affect the recall of certain aspects of memory more than others. In general, the memory of the more emotionally significant aspects of an experience is remembered better than the more emotionally benign aspects of memory (LeDoux, 1996).
With the above introduction to memory encoding and recall, let us now discuss what happens in the brain as the brain is exposed to a stimulus. All the sensory nerves (except for olfactory nerves) end up in the thalamus and are then relayed to various parts of the brain. The thalamus (which has two halves) can be thought of as brain’s switchboard or information hub. After sensory input (from eyes, ears, touch, etc.) is received and processed by the thalamus, it is sent to various cortices and to a brain structure called the amygdala. The amygdala is an almond size structure (one on each side of the brain, deep within the limbic system), which is responsible for appraisal of stimuli and evaluation of emotional significance of the stimuli. Van der Kolk (2014) calls the amygdala the “smoke detector” of the brain. If the amygdala’s evaluation of a stimulus is presence of danger, then it triggers the release of various (stress) hormones including adrenaline and cortisol, resulting in activation of the sympathetic nervous system, preparing for fight/flight or in certain situations the freeze response. Once the amygdala deems that danger is past, the body should return to its baseline state. Sensory information reaches the amygdala through two paths, which LeDoux (2002) calls the high road and the low road. I already discussed the low road, which is formed by a direct connection from thalamus to amygdala, but the high road runs through the hippocampus and anterior cingulate to the prefrontal cortex, where sensory information is processed and then sent to the amygdala (see Figure 5). For example if we see a plastic snake, our immediate reaction may be fear resulting in a defensive movement, but then within about 500 milliseconds (mSec) we may realize that the snake is plastic and harmless. This example demonstrates the low road and high road. Signals traveling through the low road reach the amygdala in less than 30~50 mSec, but the same signals traveling through the prefrontal cortex reach the amygdala in somewhere between 400~500 mSec (Siegel, 2015).
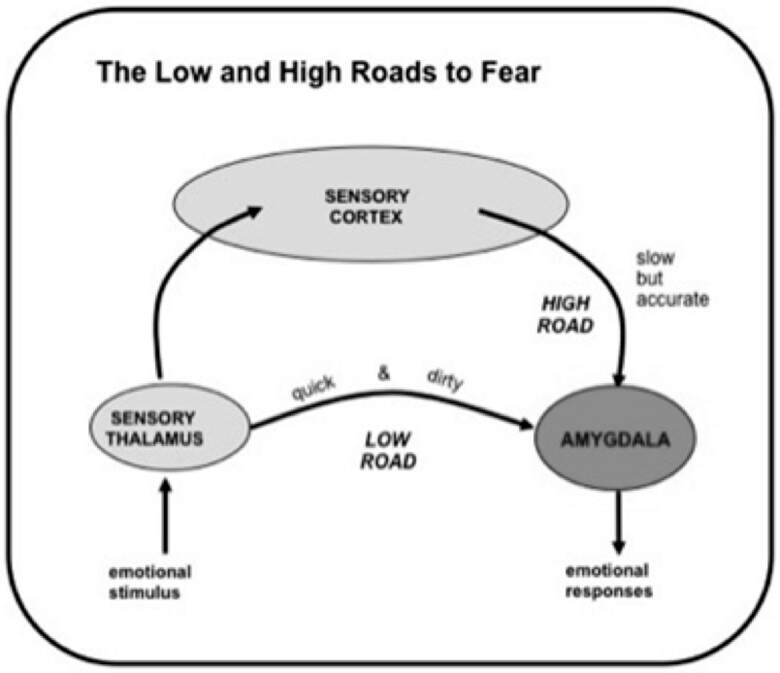
The low and high roads to Amygdala
Neuroscience of Memories – a Macroscopic View
Memory, in its most general sense, can be defined as what we consciously recall from past events. But memory is more than what we consciously recall from the past (Siegel, 1999). Siegel (1999) states, “memory is the way past events affect future functions”, (p. 24). In particular if a certain neural pattern has been activated in the past (in response to external or internal stimuli) then the probability of activating a similar pattern in the future is enhanced. This is how we remember and learn from the past. “The increased probability of firing a similar pattern is how the [neural] network remembers” (Siegel, 1999, p. 24). He further writes, “Memory storage is the change in probability of activating a particular neural network pattern in the future” (Siegel, 1999, p. 25). Our memories therefore are associated with the way these neural networks bind together to form a broader activation pattern.
Memories can be categorized in two broad categories: implicit and explicit. Implicit (procedural) memory can exist early in development and can be present at birth. Implicit memory is not subject to recall whether of self or of time (timeless). Emotional, somatosensory, and perceptual memories can be encoded as implicit memories. Generally attention is not required for encoding of implicit memories. Recall of implicit memories is independent of the hippocampus and medial temporal lobes, and thus not under conscious control (Siegel, 1999). Encoding of explicit memories begins near the second year of life, and includes semantic (factual), and episodic (autobiographical) memories. Explicit memories require conscious awareness for encoding. Explicit memories involve a subjective sense of recall and are not timeless, that is there is the notion of time in encoding of explicit memories. The hippocampus, and the temporal lobes and cortices are involved in processing and encoding of explicit memories (Siegel, 1999).
Our brain generally does not encode and save every experience as explicit memory, or else we would be inundated with so much information, such that we would not be able to function. Siegel (1999) states: “It turns out that many studies of emotion and memory point to an inverted ‘U’ shaped-curve” (p. 47). It seems that the more emotionally intense an experience is, the higher the probability of its encoding and recall. The event is simply labeled as important (by the amygdalae). Likewise, less emotionally intense events have a lower probability of being encoded and saved (Siegel, 1999). It is also important to note that events that are filled with fear, terror or are just overwhelming may not be encoded by the hippocampus. Several factors such as amygdala discharge and various neuroendocrines including noradrenaline and corticosteroids may inhibit the functioning of the hippocampus, thus blocking the encoding of the event and later recall. However, these events may be stored in implicit memory as fragments, while explicit memory is impaired (Siegel, 1999). Interestingly, when implicit memory is reactivated, it is not associated with a sense of time, place, and sense of self in time, nor is there a sense that something is being recalled. Implicit memory stores emotional dynamics of events, and not their contents. The brain can have implicit memory (mainly stored in the limbic system) from very early in an infant’s life (even prenatally). But it is only after roughly the second year of life that the hippocampus is developed enough to encode explicit memory.
It turns out that stress also mediates encoding and storing of explicit memory. Small amounts of stress generally do not have a significant effect on encoding events into memory. Moderate amounts of stress help to encode events into memory for later recall. However, large amounts of stress impair memory encoding and recall (Siegel, 1999).
Studies have shown that secretion of various neuroendocrines are involved in mediating the process of memory encoding and recall in response to stress. This process is normally transient and may last from seconds to minutes. Recent studies indicate that the HPA (Hypothalamus-Pituitary-Adrenal) axis is involved in inhibiting the functioning of the hippocampus. However, if the stress becomes chronic then it affects the size and functioning of the hippocampus, which mediates encoding of explicit memory. Chronic elevated levels of the stress hormone cortisol result in atrophy of the hippocampus. Excessive levels of epinephrine and norepinephrine (catecholamines) in response to acute activation of the autonomic nervous system (ANS) also affect encoding of memory resulting in impaired memories (Siegel, 1999). Joseph LeDoux (2002) argues that because of its connection with the hippocampus and other regions related to explicit memory system, the amygdala strengthens learned memories in the presence of emotional arousal. LeDoux (2002) further argues that as long as the degree of emotional arousal, during the memory formation is within a limit, the memory is enhanced. But if the emotional arousal goes above a limit, then formation of memory may become faulty and result in impaired memory. During a highly stressful event with high emotional arousal, the level of the stress hormone cortisol increases, resulting in interference with the functioning of hippocampus and formation of memory (LeDoux, 2002).
Traumatic Memories: Repression and Dissociation
Let us now discuss traumatic memories in more detail based on the material presented above. I indicated that if one is exposed to a highly stressful stimulus (trauma), then through activation of the amygdala and secretion of stress hormones including cortisol, the normal functioning of the hippocampus may be affected and may result in formation of impaired memory of the trauma. These memories may then be stored as isolated and dissociated fragments which can then become state dependent and get activated by sensory stimuli and emotions that are correlated with the original stressful event (trauma) (van der Kolk, 2015). It is also possible that processing in the thalamus may break down and thus the sensory information may not reach the cortices for further processing and categorization resulting in sights, sounds, smells, and touch being encoded as isolated fragments (van der Kolk, 2015). We can thus see that traumatic experience and exposure (highly stressful stimuli) may result in fragmented and dissociated memories.
LeDoux (1996) writes: “The same amount of stress that can lead to amnesia for a trauma may amplify implicit or unconscious memories that are formed during the traumatic event” (p. 246). LeDoux (1996) further discusses that the failure to recall traumatic memories may be due to amygdala mediated shutdown of the hippocampus. In this situation due to the shutdown of the hippocampus, no conscious memory might have been formed and therefore no recall can take place.
Traumatic memories may also be repressed. In fact certain aspects of traumatic memories may be repressed and other aspects dissociated. In this work however, I refer to repressed memories as those that are repressed from the conscious mind due to their unpleasant nature. It is possible that memories that may have been fragmented can also go through repression. Brewin & Andrews (1998) suggest that somewhere between 20 and 60 percent of patients in therapy who were sexually abused as children, went through periods in their lives with no recollection of their sexual abuse, and this amnesia often lasted several years. Erderlyi (2006) writes:
“Repression, conceived of as a class of consciousness-lowering processes, is divided into two sub-classes, inhibitory and elaborative processes. Inhibitory repression involves cognitive avoidance of some target material and leads to loss of accessible memory. Some of the lost memory may, however, express itself indirectly and may be partially recovered with subsequent retrieval effort. Elaborative repression distorts the original memory through a variety of transformations and false additions [fills in the gaps]” (p. 499).
Erderlyi (2006) paraphrases Freud and argues that repression originates from a highly developed ego and thus involves intention. Erderlyi (2006) also cites studies that have identified neuronal circuitries that are involved in intentional retrieval – inhibition and forgetting. These circuits involve areas within prefrontal cortices. It has also been shown using fMRI studies that prefrontal regions play an important role in suppression of emotional memories (Depue, Curran, & Banich, 2007). Depue, Banich, & Curran (2006) show that the memory representation of emotional events are encoded stronger that non-emotional events.
Anderson and Green (2001) designed an experiment called Think/No-Think in order to investigate suppression of unwanted memories. The experiment is divided in three phases. In the first phase (training) participants are presented with cue-target word pairs, and were asked to memorize the word pairs, so that when they are presented the cue they can recall the target. In the second phase (experimental), participants were asked to suppress thinking about corresponding targets when presented with certain cues (no-think condition), while they were asked to think about corresponding targets when certain cues were presented (think condition). And in the final phase of the experiment memory recall of corresponding targets for each cue was assessed. Using the experiment designed by Anderson & Green (2001), Depue, Banich, & Curran (2006) further found that in Think/NO-Think experiments designed to achieve suppression, the recall of emotional memory was seen to be greater that non-emotional memory in the Think experiment, and the reduction of recall for emotional memory was smaller in the No-Think experiment.
Thus emotional memories would go through stronger encoding. It is therefore more difficult to suppress intruding thoughts related to highly stressful events, as is the case in those who suffer from PTSD. Erdelyi (2006) asks the question whether emotionality enhances or degrades memory, and the answer that is given is yes and yes. The author explains, “There is widespread consensus that emotionality enhances memory for central elements of stimuli but degrades memory for peripheral items” (p. 503). It is important to note that memory in general is a heterogeneous construction and what applies to one aspect of memory may not apply to other aspects (Erdelyi, 2006). Thus, it is possible for certain aspects of memory to be fragmented and dissociated due to the level of stress associated with the stimuli, while less important and peripheral aspects may be repressed by conscious memory and forgotten.
Howell Compares Repression and Dissociation
On the subject of repressed vs. dissociated memories, Howell (2005) compares and contrasts repression and dissociation:
- Repression is both motivated and defensive. In contrast, dissociation does not have to be motivated or psychologically defensive. For example, dissociation can arise automatically in the moment of trauma, or non-defensively in response to hypnosis.
- Repression refers to formulated experience, and dissociation generally refers to unformulated experience.
- Repression usually refers to a piece of information that was accessible at one time but not at another, whereas dissociation usually refers to divisions of experience in which the parts are side by side, contrasting, and may be concurrent in time. Dissociation refers to states and systems of states, which are often mutually exclusive.
- Dissociated memories are especially context-dependent. (p. 198)
In repression unacceptable psychic content is pushed down into the unconscious, while in dissociation the split-off and dissociated content is not out of sight permanently or continuously but can reappear at any time due to external or internal stimuli. Freud was hypothesizing that repressed material is converted in alternatives such as dreams, slips, and symptoms, etc., while Erdelyi (2006) and van der Kolk (1994) argue that alternative modes of remembering are not conversions, but are spared memories. Erdelyi writes, “By this view, repression knocks out declarative (conscious) memories, but other memory systems (e. g., procedural ones, as in symptoms) are not similarly affected and continue to reflect remembering” (Erdelyi, 2006, p. 507).
Freud versus Janet on Trauma Memories as Repressed or Dissociated
There have been disagreements between researchers as to whether traumatic memories are repressed or dissociated in nature. This debate and discussion is not new and originates from the historical disagreement between Freud and Janet. Freud believed that memories of trauma, and he was specifically referring to hysterics, are repressed, while Janet was of the belief that traumatic memories are dissociated. Of course both Freud and Janet were writing about hysterical phenomenon, and it is particularly the hysterical phenomenon that may share aspects of both repression as well as dissociation. Freud (1952c) believed that the major motivation for repression is avoidance of pain. He also indicates that the essence of repression is to keep something painful out of consciousness. While Janet thought that intense emotions can cause dissociation of memories from consciousness. These dissociated memories are then stored as visceral sensations, or as visual images (flashbacks) (van der Kolk, 1994).
Afferent Neurons, Memory and fMRI
In shock trauma, the signals from afferent neurons (sensory neurons) may not fully reach the cortex to be processed, neither can the hippocampus categorize, organize, and encode the memories. Therefore these memories may not be recalled as a complete whole, but only are recalled as fragments and tend to be associated with sensory inputs, and certain body states, which may include sounds, imagery, touch, and certain body positions, etc. (Siegal, 1999). What happens, as I indicated earlier, is that signals from afferents (sensory nerves) take about 30~50 milliseconds to reach the limbic system (and the amygdala), but the same signals take much longer, that is of the order of 500 milliseconds to reach the frontal cortex to be processed. This is an evolutionary advantageous process, as in the face of an attack by a predator, our ancestors needed to act immediately, or else they would have been killed. In the face of massive trauma, the neuropathways from the limbic system to the cortex are blocked. The memories retained in the limbic system are timeless and can be activated at any time due to certain stimuli, and the patient’s perception is that the memory fragments correspond to “now”, due to the timelessness of such memories. Furthermore, memories are stored in different functional parts of brain, and are organized later by the hippocampus and processed by the prefrontal cortex (PFC). Recent fMRI techniques have shown that there is an inverse correlation between activation of the amygdala and the right prefrontal cortex.
Recent studies in neuroimaging have also indicated that the dorsalateral and ventralateral prefrontal cortices (DLPFC, and VLPFC), as well as the anterior cingulate cortex (that is connected to the prefrontal cortex – PFC) and pre-supplementary motor cortex, are all involved in repression of painful memories. In contrast, activities in the hippocampus, a region of the brain crucial to encoding of explicit memory were reduced (Anderson, et al. 2004). This result was also shown in a separate study conducted at the University of Colorado, Boulder (2007) by Depue and Curran, which measured brain activities in subjects who were trained to repress painful memories, and memories of negative images. Depue, Banich, & Curran (2006) have found that the suppression of unwanted memories occurs along two pathways, and write:
“The first pathway involves cognitive control by the right inferior frontal gyrus (rIFG – part of the lateral frontal lobe) over sensory components of memory representation … This finding is consistent with computational models that posit that activation and inhibition of the thalamus is a critical means of gating (blocking) working memory information. A second pathway involves cognitive control by the right middle frontal gyrus (rFMG – part of the lateral frontal lobe above rIFG) over memory processes and emotional components of memory representation via modulation of hippocampus and amygdala.” (p. 218)
Limbic System, Implicit Memory and Elaborative Repression
It is however, important to note that emotional aspects of the traumatic memories are stored as implicit memories in the limbic system. There is thus a splitting off or dissociation of contents of the painful experiences from the emotional aspects and dynamics of the experiences. The painful contents are repressed while the emotional dynamics are retained as implicit memories. As Shore (1994) indicated this splitting process is inter-hemispheric as well.
It is also important to mention that the recall of (degraded) past memories recovers some parts of these memories but may further augment these memories for meaning (elaborative repression), in an effort to reduce the uncertainty, and increase predictability in order to reduce arousal (Erdelyi, 2006). In dissociation however, this same process may not occur, as these memories are highly state dependent and typically are not amenable to augmentation the way repressed memories may be. This is partially due to the nature of the dissociated memories that overwhelm various neuronal circuits and block the normal processing of these memories. Ledoux (1996) writes:
“… if the hippocampus was completely shut down by the stress to the point where it had no capacity to form a memory during the event, then it will be impossible through any means to dredge up a conscious memory of the event. If no such memory was formed, then no such memory can be retrieved or recovered. On the other hand, if the hippocampus was only partially affected by the trauma, it may have participated in the formation of a weak and fragmented memory. In such a situation, it may be possible to mentally reconstruct aspects of the experience. Such memories will by necessity involve “filling in the blanks”, and the accuracy of the memory will be a function of how much filling in was done and how critical the filled-in parts were to the essence of the memory” (p. 244).
Gluing Dissociated Memories
However, it may still be possible to “glue” the dissociated memories together to make some sense of them, and to reduce arousal. However, for this gluing of dissociated memories to be possible, clients must be able to tolerate high arousal and not be overwhelmed, while the narrative is being reconstructed. We, as bioenergetic therapists are fully aware that the presence of an empathic, supportive, and attuned therapist is a crucial stem in this process. This form of client-therapist connection allows clients to make left hemisphere centric sense of their right hemisphere representations, resulting in the capacity to regulate strong emotional states (Siegel, 1999). The presence of an empathically attuned therapist may keep the clients arousal within a tolerable level, causing the integration of traumatic memories.
In summary, it is clear that empathic attunement and limbic resonance in the therapeutic relationship is a necessary requirement for treatment of trauma whether traumatic memories are repressed or dissociated. The therapist must be emotionally attuned to his patients and let them regulate their strong affects within the therapeutic relationship. This means that the therapist must also be able to contain those same affects (Hilton, 2007). Traumatic experiences and memories cause us to split from our integrated and spontaneous selves. And it is the presence of an empathically attuned therapist that can give us the possibility of recovery and integration. We can then become free, and not be haunted by nor enslaved by traumatic memories (Hilton, 2007).
Case of Elizabeth
Elizabeth (name changed for confidentiality) was an attractive woman in her thirties. She came to see me due to severe anxiety. She was highly educated and was pursuing post-graduate studies in science. Her body was rigid with some oral characteristics. Elizabeth did not describe herself as an anxious person but said that over the last few weeks, before coming to see me, she had been very anxious and concerned about her health. Specifically, she feared that she had cervical cancer. She had seen her physician who had observed an anomaly in her blood test and wanted her to come back for more tests. My first recommendation to her was to see her gynecologist, which she did and it turned out that her anxiety was baseless. However, her anxiety continued as she was not satisfied with the test results. She continued to believe that she had a serious disease related to her sexual organs. After a number of sessions working with her on her anxiety and getting her family history, I felt that the therapeutic connection and relationship was established. I was nearly of the same age as this client’s father, and a strong positive father transference had also established. The first few sessions were mostly conducted around taking a history, having the client breathe deeply and ground. I also explored with her if she felt her pelvis. Her answer was “no”! In fact she felt that part of her body somehow was not clean and she essentially had dissociated from her vagina and pelvic area.
From the very first session, I noticed that Elizabeth, when listening to me, turned her head slightly to the right and looked at me from the corner of her eyes, as if she did not trust me. Also her right arm was essentially immobile while she sat on the couch, but her left arm was fairly animated. Her legs were very close together and her right arm, while immobile gave the impression that she was covering her vagina. When I felt that a strong therapeutic relationship was established, I decided to go a little deeper, and brought my observations to her attention. I asked her to see what happens if she perturbed those movements and positions of her limbs, as well as listening to me while she was directly looking at me. She immediately recognized that she did not fully trust me yet, but did not know why, as there was no reason in her mind not to trust me. However, when she put her arms to her side, she immediately felt very anxious, especially as she relaxed her legs.
She then shared with me a story that she had not shared with anyone. She mentioned that shortly after she started working with me she became aware of sexual abuse by an older cousin that occurred when she was 5 or 6 years old. She felt those memories were dreamlike and she was not sure if they had actually happened. This cousin was a favorite of hers and she looked up to him with great respect and admiration.
As she told this story, Elizabeth became anxious. I asked her what sensations she had in her body, and she said that her legs felt really cold. I asked what her body wanted to do. She replied she wanted to stand up. I asked her to follow her instinct and do so and keep her knees slightly bent. Her legs started vibrating. She started crying and expressed that she was very scared. She did not want to share her memories that had just come up. I mentioned to Elizabeth that of course it was okay not to share the memories, but it would be great if she felt safe enough to stay with them. She reported that she felt safe and could stay with the memories that had just surfaced. I asked if she had been alone with the perpetrator. She replied “yes”, and that the two of them were alone in her cousin’s house. I asked her if she was aware whether she was in a room and where the door was. She mentioned that she was aware and I asked if she could run toward the door, open it and run out. In her imagination she did that, and found herself in an alley outside the house but alone which was scary for her, as he could follow her and catch her. I asked her if there was a store around. She replied “yes” there was a small grocery store around and I asked her to run there and stay as she was safe there.
Her fears then subsided but her body was shaking and discharging trauma. I had read in one of Peter Levine’s (2003) articles that he had intervened in a similar way for a man who was attacked by wild dogs. My intervention was influenced by what I had read in Levine’s work. The session was coming to an end and we had gone over by some time. Since she was my last client that day, I stayed with her until Elizabeth’s nervous system calmed down.
The following session mostly revolved around processing what had happened in the previous session. Elizabeth still did not feel she could share what actually had happened, and I again normalized her feeling, in that it was not necessary to share if she did not want to. In the next session, I asked Elizabeth if she wanted to do more work with her trauma, and she replied “yes”. Again, I asked her to feel her body, her legs in particular and her right arm (which was immobile), while she became aware of the memories. Her legs started vibrating very quickly and she spontaneously stood up and her vibration got stronger. This time her right, previously immobile forearm, started to rotate around the elbow. The rotation got a bit more intense, and while this was going on I noticed that her weight tilted to the right and the left side of her right foot was slightly lifted off the ground.
It gave the impression that someone was twisting her arm behind her back. I shared my observation with her. She then started sobbing and was very fearful. She did not share the memory that had come up, but I asked her if her right arm was twisted behind her back while the abuse was going on. She mentioned that it was the case, but this time she was much more fearful and scared. She was shaking and sobbing.
Elizabeth was becoming dysregulated and I could not intervene the way I did two sessions prior. This time I asked to her to hold on to my forearm (for more support) so that we could run together and that I would be with her as she runs for safety away from the house and the perpetrator. We “ran” together to the same grocery store that she imagined before. This time I told her that I would stay with her for as long as necessary until her parents came back and until she felt safe. Her nervous system calmed down after several minutes followed by more shaking and sobbing.
The work with Elizabeth is continuing and she is progressing well. She has been working with me for about 8 months. In one session two months ago, she mentioned that one of her colleagues was inappropriate with her, especially when she visited him in his office and that she froze and could not move or say, “NO”. We worked on setting boundaries and saying “NO”. I asked Elizabeth what it was that she could do if the colleague could not hear “NO”, and did not respect her wishes. She very quickly and spontaneously said: “Of course I can run away”. Elizabeth has been empowered since that session, is dating someone now, is discovering herself and her sexuality again, and the memories of the trauma have lost their grip on her.
This case demonstrated dissociation as well as the repression of traumatic memories. Elizabeth did not remember the abuse and then only as a dreamlike memory which she was not sure was real. We started from her body, her sensations and feelings to recover and integrate the fragments. But as I discussed earlier, recalled memories are the highly worked over version of the original encoded memories and go through transformation. Hence, we augmented her memories by empowering her and enabling her to run away, which included completing the actions that were blocked at the time of the trauma. The newly formed memories, although containing the original painful aspects, now were augmented by the empowering memories as well. My hope is that over time these newly formed memories will become her default memories. In other words, we were able to glue the fragmented and dissociated memories of the abuse with new memories that empowered Elizabeth, reduced her arousal and lowered the activation of her amygdala. This approach is further confirmed in a recent study by Díaz-Mataix, Ruiz Martinez, Schafe, LeDoux, & Doyère (2013) who showed that it might be possible to trigger synaptic plasticity and reconsolidation of aversive memory in the lateral amygdala (LA) by introducing new information at the time of recall and reactivation.
Case of John
John (name changed due to confidentiality) was a man in his late forties. He came to see me because he had just changed jobs and found himself in a very anxious place. His anxieties were on the verge of becoming panic attacks. He said he would wake up in the middle of the night sweating and was very anxious in the morning once he woke up. He was also showing signs of mild depression. This was not the first time that John had faced anxiety and depression. It seemed like any time he was in a situation in which the stakes were high (as in possibly not performing well and losing his job), he ended up with anxiety and eventually depression. He described how he experienced the same symptoms (even stronger than now) 10 years ago when his business had to file for bankruptcy and he had to be hospitalized for several days. John was an educated man who was very rigid and very obstinate. His jaw was very tense, such that he could hardly open his mouth. His lower back was also very tense and contracted. When I pointed these out to him, he agreed. He mentioned that as a result of the tightness in his jaw, he had destroyed many of his teeth and had muscle spasms in his lower back frequently! I asked John for his memories of his childhood and what he remembered. I usually ask this question right after I hear the presenting issue.
The idea behind this is that due to the associative nature of memory, there is a strong likelihood that childhood memories and experiences that are responsible for present day behaviors and conflicts get activated, and the client can describe them as they are closer to conscious recall. John mentioned that he was the youngest in a family of 6 siblings. He shared that his father, for as long as he remembered, was severely depressed, was not working, stayed at home essentially most of the time, and passed away when John was 10 years old. His mother, on the other hand was working two jobs to make ends meet. She essentially was a single mom and the only breadwinner, although as John’s older siblings became old enough to work, they helped as well. John remembered that his family had to move many times, as the family could not afford the rent, would fall behind and get evicted.
John never felt secure and was anxious as a child. He remembered the worried look on his mother’s face, not knowing what he should do and getting more anxious and scared. John is the most educated in his family and when he was 16 he left his household and started to work, went to school, and eventually became successful. He also brought his mother to live with his family when he married his wife, and essentially took care of her until she died. It took many sessions for John to realize the connection between his earlier experiences in life and his present day symptoms. We moved very slowly and I mixed analysis and interpretation with bodywork (grounding and breathing), while we were building a strong therapeutic relationship.
On one occasion John called me half an hour before his session to cancel. I was somewhat upset and told him, perhaps in a harsher tone than my usual, that he should have let me know at least a day in advance. He missed the following session as well. When he eventually came back, I felt that what had happened between us had to be processed. John mentioned that he expected me to ask why he was canceling and felt that I did not care for him as much as he thought I did, otherwise I would have asked him why he was not able to make it to his session. I said to him I was sorry for letting him down. He replied that he was very depressed, was feeling really down and that was why he could not make it to his session and had to cancel. That session was mostly spent on processing what had happened which turned out to be crucial, as the positive transference had turned into strong a negative transference. I also expressed how sorry I was that he was stricken by severe depression and anxiety on the day that he canceled his session. We were able to mend the rupture, and rebuild a very strong therapeutic relationship.
John was showing signs of improvement and feeling less anxious albeit at a slow pace. In one session, several months ago, John said that he was taking a couple weeks off, would travel and would like to spend time with his children and other close relatives. I was very encouraging of this plan, as in general John did not have strong connections with his family or friends. When he came back, much of the work we had done had solidified and he was and continued to feel much better, with his anxiety mostly gone. The new neural pathways that were being laid out in our connection and work were finally activated and had become the default pathways, in the Hebbian sense. The new pathways had taken hold and his new experience of being seen for who he was nonjudgmentally with empathy, understanding, and affection were the crucial catalysts for his change. John had never experienced this and it was this kind of connection that created the facilitating and holding environment for him to be able to tolerate the affects related to his earlier experiences and to integrate them. Much work still needs to be done, as his body still manifests strong holding. This case presented a situation in which there was dissociation between the narrative (story), and the affects related to earlier developmental trauma. The affects were repressed but the explicit memories of the experience were retained. However, John was repeating and recapitulating the earlier traumas, despite the dissociation and repression.
Conclusion
In this paper, a detailed description of formation of memory based on neuroscience was given. Different types of memories were reviewed, while definitions of repressed memories and dissociated memories were introduced. Formation of dissociated memories as well as mechanisms of repression of memory based on recent fMRI studies and neuroscience research, were discussed. It was argued that traumatic memories frequently have dissociated aspects and repressed aspects. It was concluded, and shown, based on recent research in neuroscience that regardless of the nature of traumatic memories, a very important factor in the treatment of trauma was the presence of an attuned therapist in the therapeutic relationship. Finally, two case studies were presented to highlight the arguments set forth in this paper.
References
Anderson, M. C., & Green, C. (2001). Suppressing unwanted memories by executive control, Nature, 410, 366–369.
Anderson, M. C., Ochsner, K. N., Kuhl, B., et al. (2004). Neural systems underlying the suppression of unwanted memories. Science, 303, 232–235.
Brewin, C. R., & Andrews, B. (1998). Recovered memories of trauma: Phenomenology and cognitive mechanisms. Clinical Psychology Review, 18, 949–970
Depue, B. E., Banich, M., & Curran, T. (2006). Suppression of emotional and nonemotional content in memory: Effects of repetition on cognitive control. Psychological Science, 17(5), 441–447.
Depue, B. E., Curran, T., & Banich, M. (2007), Prefrontal regions orchestrate suppression of emotional memories via a two phase process, Science, 17, 215–219.
Díaz-Mataix L, Ruiz Martinez R. C. et al. (2013). Detection of a temporal error triggers reconsolidation of amygdala-dependent memories. Curr. Biol. 23(6): 467–472.
Erdelyi, M. H. (2006). The unified theory of repression. Behavioral and Brain Sciences, 29, 499–551.
Freud, S. (1952a). Beyond the pleasure principle. Major works of Sigmund Freud. (pp. 639–663). London, England: Encyclopedia Britanica, Inc.
Freud, S. (1952b). Selected papers on hysteria. Major works of Sigmund Freud. (pp. 25–115). London, England: Encyclopedia Britanica, Inc.
Freud, S. (1952c). Repression. Major works of Sigmund Freud. (pp. 59–81). London, England: Encyclopedia Britanica, Inc.
Hebb, D. O. (1949). The Organization of Behavior: A Neuropsychological Theory. New York: Wiley and Sons.
Hilton, R. (2008). Relational somatic psychotherapy. M. Sieck (Ed.). Santa Barbara, CA: Santa Barbara Graduate Institute.
Howell, E. F. (2005). The dissociative mind. New York, NY: Routledge.
LeDoux, J. (1996). The emotional brain. New York, NY: Simon & Schuster.
LeDoux, J. (2002). Synaptic self. New York, NY: Penguin Books.
Levine, P. (2003). Panic, biology, and reason: giving the body its due. The USA Body Psychotherapy Journal, 2003, 2(2), 5–14.
Siegel, D. (1999). The developing mind. New York, NY: Guilford Press.
University of Colorado at Boulder (2007, July 12). Emotional Memories Can Be Suppressed With Practice, Study Says – (Brendan Depue & Tim Curran). Science Daily. Retrieved 2011: http://www.sciencedaily.com/releases/2007/07/070712143304.htm
Van Der Kolk, B. (n. d.). Developmental trauma disorder. Retrieved from:
http://www.traumacenter.org/products/pdf_files/preprint_dev_trauma_disorder.pdf.
Van Der Kolk, B. (1994). The Body Keeps the Score: Memory and the evolving psychobiology of post traumatic stress. Harvard Review of Psychiatry, 1994, 1(5), 253–265. Retrieved 2011: http://www.traumapages.com/a/vanderk4.php
Van Der Kolk, B. (2014). The Body Keeps the Score: Memory, mind, and body in the healing of trauma. New York, NY: Viking.
About the Author
Homayoun Shahri, Ph.D., M. A., LMFT, received his PhD in electrical engineering from Lehigh University in 1990, and his master of arts in clinical and somatic psychology from Santa Barbara Graduate Institute (now part of The Chicago School of Professional Psychology) in 2012. He is a licensed marriage and family therapist, and has a private practice in Irvine, CA, USA. Homayoun completed the Bioenergetic training program in the Florida Society for Bioenergetic Analysis in 2009. He is a member of the Southern California Institute for Bioenergetic Analysis (SCIBA), where he is working toward the completion of his certification requirements. Homayoun is a member of the United States Association of Body Psychotherapy (USABP), International Institute for Bioenergetic Analysis (IIBA), and California Association for Marriage and Family Therapists (CAMFT). He is on the peer review board of the International Body Psychotherapy Journal (IBPJ).