The Borderline Client, Shame and Somatic Counter-Transference
Ingrid Cryns
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2017 (27), 111–156
https://doi.org/10.30820/0743-4804-2017-27-111 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstracts
English
This paper is about understanding possible source causes of Borderline Personality Disorder (BPD) and how it differs from Bipolar Disorder (BP), Narcissistic Personality Disorder (NPD), Post Traumatic Stress Disorder (PTSD) and Attention Deficient/Hyperactivity Disorder (ADHD). The distinctions can be hard to grasp, are often overlapping, co-occurring at times and/or possibly mis-diagnosed. An overview is offered that compares the similarities and differences between these conditions. The core affect of shame is explained in how it may be experienced somatically in a Borderline client and the relationship of shame to distinct negative feelings of disgust, abandonment, and rejection are discussed. When working with difficult emotional states, some ideas are presented to work as a body oriented (Bioenergetic) psychotherapist to support a more integrated healing and recovery program for a BPD client. Some suggestions of diet, supplements and natural remedies are also included. Finally, recommendations are presented regarding how a psychotherapist can track and understand their own somatic counter-transference issues in order to work more effectively with a BPD client.
Key words: Borderline, Shame, Trauma, Somatic Counter-transference, Negative Feeling Affects
German
Dieser Beitrag bemüht sich um ein Verständnis möglicher ätiologischer Faktoren für die Entstehung von Borderline-Persönlichkeitsstörungen (BPS) und wie sich diese von Bipolaren Störungen, Narzisstischen Persönlichkeitsstörungen, der Posttraumatischen Belastungsstörung (PTBS) und der Aufmerksamkeits-Defizit/Hyperaktivitätsstörung (ADHS) unterscheiden. Die Unterscheidungen sind zum Teil schwer fassbar, die Störungsbilder überlappend; manchmal treten sie als komorbide Störungen auf und/oder werden fehldiagnostiziert. Es wird eine Übersicht zum Vergleich von Ähnlichkeiten und Unterschieden zwischen diesen Störungsbildern gegeben. Der Kernaffekt der Scham wird als somatisches Erleben bei einer Borderline-Patientin beschrieben, und es wird der Zusammenhang zwischen Scham und den klar unterscheidbaren negativen Gefühlen des Ekels, der Verlassenheit und der Ablehnung diskutiert. Für die Arbeit mit schwierigen emotionalen Zuständen werden einige Vorschläge gemacht, wie man als körperorientierte (bioenergetische) Psychotherapeutin ein integratives Heilungs- und Genesungsprogramm für eine Patientin mit BPS unterstützen kann. Schließlich werden Empfehlungen formuliert, wie ein Psychotherapeut eigene somatische Gegenübertragungsthemen kontinuierlich beobachten und verstehen kann, um effektiver mit BPS-Klient/innen zu arbeiten
Italian
Questo articolo cerca di comprendere le possibili cause alla base del disturbo borderline di personalità e come questo si differenzia dal disturbo bipolare, dal disturbo di personalità narcisistico, dal disturbo post traumatico da stress (PTSD) e da quello di deficit di attenzione/iperattività. Le distinzioni possono essere difficili da afferrare, ci sono spesso sovrapposizioni, comorbilità, e/o a volte, errori nella diagnosi. Viene offerta una panoramica che confronta le somiglianze e le differenze tra queste condizioni. L’affetto centrale della vergogna viene spiegato per come sperimentato a livello corporeo da un cliente borderline e viene approfondito il rapporto della vergogna per distinguere i sentimenti negativi di disgusto, abbandono e rifiuto. Vengono presentate alcune idee, utili quando si lavora con stati emotivi difficili, per lavorare come psicoterapeuti corporei (bioenergetici) e sostenere un programma di recupero di guarigione integrato per un cliente BPD. Infine, vengono presentate delle raccomandazioni che aiutino lo psicoterapeuta a monitorare e comprendere i propri problemi corporei di controtransfert, al fine di lavorare in modo più efficace con un cliente BPD.
Spanish
Este ensayo consiste en entender las fuentes posibles de las causas del Trastorno de la Personalidad Borderline (TPB) y cómo se diferencia del Trastorno Narcisista de la Personalidad (TNP), del Trastorno Bipolar (TB), del Trastorno de la Deficiencia de la Atención e Hiperactividad (TDAH), y del Trastorno de Estrés Postraumático (TEP). La distinción puede ser difícil de captar porque a menudo se sobreponen, concurren y a veces, o posiblemente se mal diagnostican. Se ofrece un resumen que compara las similitudes y diferencias entre estas condiciones. El sentimiento base de la vergüenza se explica desde el punto de vista de la experiencia somática de un cliente con trastorno de personalidad Borderline y se plantea la relación de la vergüenza para diferenciar sentimientos negativos de asco, abandono y rechazo. En la intervención con estados emocionales difíciles, se presentan algunas ideas para trabajar como un terapeuta de orientación somática (Bioenergética) y así mismo apoyar la curación integral y un programa de recuperación para un cliente TPB. Por último, se presentan recomendaciones acerca de cómo un psicoterapeuta puede seguir y entender sus propios problemas de contratransferencia somática para trabajar más eficazmente con un cliente TPB.
Portuguese
Este artigo é sobre o entendimento de possíveis causas da fonte da Desordem de Personalidade Borderline (BPD) e de como ela difere da Desordem Bipolar (BP), da Desordem da Personalidade Narcisista (NPD), da Desordem do Estresse Pós-Traumático (PTSD) e da Desordem da Deficiência de Atenção/Hiperatividade (ADHD).
Essas diferenças podem ser difíceis de compreender e frequentemente se sobrepõem, ocorrendo às vezes simultaneamente e/ou sendo mal diagnosticadas. Mostra-se, também, uma visão geral que compara semelhanças e diferenças entre essas condições. Focaliza-se o afeto central da vergonha como experienciado somaticamente no cliente Borderline e discute-se a relação da vergonha com diferentes sentimentos negativos como nojo, abandono e rejeição. Ao trabalhar com estados emocionais difíceis, algumas ideias são apresentadas para ajudar o psicoterapeuta de orientação corporal (Bioenergética) a dar suporte a um programa de tratamento e recuperação integrado para o cliente BPD. Finalmente, apresenta-se algumas recomendações sobre como um psicoterapeuta pode descobrir e entender suas próprias questões de contratransferência somática, no sentido de trabalhar mais efetivamente com um cliente BPD.
Introduction
For many individuals that are diagnosed Borderline Personality Disorder (BPD), the core root has been theorized as insecure early attachment with a primary caregiver, which this paper briefly explores. Early attachment disruption for BPD clients may be affected by disorganized patterns or paradoxical triangulations of early family interactions. One example is in the absence or confusion of the essential interactive role of the father (or secondary caregiver) in the Primary Triangle relationship between mother, father and child1.
BPD may also develop outside of insecure early attachment bonding. There is some evidence of a more ‘sensitive’ genotype that may be inherited2 3 (Linehan, 1993, Stepp, 2011). This sensitivity may also be linked to traumatic environmental influences such as, “sexual and physical abuse, parental divorce or illness or parental psychopathology”4 (Distal, 2009). Experiencing trauma through war, accidents, or peer bullying for some individuals may also cause decreased ability to respond well to environmental stresses and thus become a pre-disposition to higher risk for developing BPD symptoms. Adolescents that have had childhood bullying or difficulties with peer relationships have been found to have an increased risk factor for developing BPD5 6 (Kaess, 2014, Woke, 2012). This risk may be exacerbated by the brain development that occurs during this period.
There is more recent research that indicates there may be brain abnormalities in the pre-frontal cortex (PFC) and the amygdala in BPD individuals that explains their difficulty with negative emotions, heightened impulsivity and the struggle to modulate their emotions in healthy ways for themselves7 (Weill Cornell Medical Center, 2007). This creates a central core issue of a non-cohesive self-image where there can be an incongruent continuum of feelings of shame, disgust, abandonment, and/or rejection of their sense of self.
A brief note about the DSM diagnosis labels: The DSM was originally created as a way to accurately prescribe pharmacology support to help patients manage presenting symptoms so as to not suffer. It also provides a base with which to discuss with other clinicians issues of common understandings. However, diagnostic labels can also be very limiting in terms of accurately describing the complex characteristics of a distressed or suffering individual. For the purposes of this paper, the intent of its use is to be able to describe some of the larger issues that individuals may have. The focus is to differentiate more clearly what is characterized mostly as BPD and the difficulties in distinguishing the BPD way of relating to the world. It is important to note that all individuals can be understood along a dimensional continuum of severity of ego functioning, with a great variety of strengths and weaknesses.
The recovery prognosis of BPD can be very promising if understood in terms of how to work with the inter-connectedness of the body and mind, how to regain the capacity for biological self-regulation, how to reform the relational attachments, and how to cooperate with other people. It is important to also note that this is long-term therapy that requires a commitment as well as the ability to be able to follow through with treatment suggestions.
It is the right brain, non-verbal processing that creates the ability to connect the physical and emotional experiences with the mind’s conscious awareness8 (Resneck-Sannes, 2002). The brain can continuously change through teaching new body connections and sensory awareness, as well as new methods of how to bring the body back into regulation from disconnected, confused, incoherent or chaotic states (due to emotional, unconscious, and/or dissociated triggers).
A body-based form of psychotherapy, such as Bioenergetic Analysis, is uniquely placed to work with re-establishing a secure, relational attachment (with the therapist) though the non-verbal, somatic information system and integrate it into a new consciousness of safe, consistent connection with self, with others, as well as ways of how to cooperate with others. Long term therapy with a body oriented psychotherapist, familiar with how to work with the subtle hiding, splitting off or dissociated aspects of BPD, can help to reform the neural network pathways and neurobiology within a BPD client.
BPD Concepts & Diagnostic Criteria
Imagine that your core sense of self feels like it is a cylinder of Swiss cheese, with the holes, rips or tears as the missing, fragmented pieces of their solid sense of self.
Or that your sense of self is like a series of separate islands of consciousness that switches or leaps from one island to another, missing a solid connection or bridges holding them all together. This is what the internal organization of a client with Borderline Personality Disorder is like. It is a complex and often difficult disorder to fully comprehend.
BPD is essentially about emotional affect dysregulation and how that ultimately creates an unstable and non-cohesive sense of self. The core structural essential disturbances that are commonly suggested for BPD are9:
- A pervasive pattern of disturbed or unstable interpersonal relationships
- Affective or emotional dysregulation, and
- Behavioural impulsivity or dys-control by early adulthood
What is very significant in BPD clients is an extreme fear of abandonment. This fear is an unconscious driving impulse that contains rejection along with extreme shame and disgust about their sense of self. These clients often have poor interpersonal relationships and behaviour impulsivity caused by constant intense triggers (perceived or real) and the consequent emotional dysregulation in response. Other preferable names have been suggested for BPD, such as ‘Emotional Dysregulation Disorder’ or ‘Emotional Regulation Disorder’ 10 (Gunderson 2005), which may be preferable when speaking with clients and their families.
The following is a Basic Checklist of BPD symptoms (A minimum of 5 out of 9 Symptoms according to the DSM-IV-TR11 is required and some points from DSM-512 are also integrated with extra descriptions).
- An intense fear of abandonment or being left alone. [Separation insecurity: Fears of rejection by – and/or separation from – significant others, associated with fears of excessive dependency and complete loss of autonomy. (This can be real or imagined, sometimes seen as a high need to do everything together, or desperate efforts to hold onto the other person, or acting out rejection of others before they get rejected themselves)]
- A pattern or history of unstable and intense, conflictual relationships [Impairments in interpersonal functioning through empathy (compromised ability to recognize the feelings and needs of others with interpersonal hypersensitivity {i.e., prone to feel slighted or insulted}; perceptions of others selectively biased toward negative attributes or vulnerabilities) and/or intimacy {mistrust, neediness, and anxious preoccupation with real or imagined abandonment, close relationships often viewed in between extreme swings (seeing others as all good) or devaluation (all bad) and alternating between over involvement and withdrawal.]
- An identity disturbance, or low sense of self worth [A persistently unstable or unclear sense of their self-image, impairment in self functioning, often associated with excessive self criticism, poor self-direction: instability in goals, aspirations, values or career plans]
- Impulsive, Disinhibition and/or self-destructive or sabotaging behaviours [Acting on the spur of the moment in response to immediate stimuli or acting without a plan or consideration of consequences, denial of reality of personal danger, as seen in at least two areas such as reckless driving, out-of-control spending, substance abuse, sex, or binge eating, etc.]
- Recurrent self-harming behaviours [such as threats, gestures, self-cutting, burning, skin scratching, hair pulling or repeated suicidal impulses]
- Extreme emotional affect instability [Unstable mood swings, easily aroused & reactivity out of proportion to events and circumstances with alternating states of intense negative feelings such as: episodic dysphoria (depression, sadness, misery, hopeless, pessimistic about the future, pervasive shame, feeling of inferior self-worth and difficulty to recover from these moods), irritability or anxiety (nervousness, tenseness, or panic, worry about past or future, apprehensive, threatened by uncertainty, fears of falling apart or losing control) lasting often from a few hours to (rarely) a few days]
- Chronic feelings of emptiness
- Inappropriate, intense, explosive anger reactions [Persistent or frequent anger in response to minor slights and insults and/or a difficulty controlling anger such as constant angry outbursts, recurrent physical fights, frequent displays of temper, etc.]
- Temporary states of losing a sense of reality or paranoid thoughts [that can be triggered by stress, food or medications and causes severe dissociative symptoms (psychosis)]
According to the DSM-5, it is important to note that there are 3 further criteria traits to consider13:
- The impairments in personality functioning and the individual’s personality trait expression are relatively stable across time and consistent across situations.
- The impairments in personality functioning and the individual’s personality trait expression are not better understood as normative for the individual’s developmental stage or socio-cultural environment.
- The impairments in personality functioning and the individual’s personality trait expression are not solely due to the direct physiological effects of a substance (e. g., a drug of abuse, medication) or a general medical condition (e. g., severe head trauma).”
Some BPD individuals may have an inability to hold separateness with the ‘other’ in their sense of self and their core fear of abandonment and/or rejection. In general, BPD individuals tend to have a poor sense of boundaries. This may be observed externally in leaving doors open, poorly organized closets, drawers or refrigerators; living with a lot of clutter, hoarding or difficulty letting go of personal possessions (attachment displacement); feeling threatened by differences or alternative points of view; a great difficulty saying ‘No’ to others; or a difficulty making sound decisions. Other BPD individuals may also have an inability to hold an inner sense of constancy with others that is reliable and trustworthy. Defined as a lack of ‘object constancy’14, when an ‘other’ is not physically present with them, they find it difficult to hold their image or sense of connection with them.
Reality for many BPD clients can feel like walking on sand that is constantly shifting. It never feels like their reality feels stable or solid. Typical phrases describing or generally felt by BPD clients can be any of the following:
“I hate you but I can’t leave you.”
or
“I hate you – don’t leave me.”15
“I’m so good at the beginnings, but in the end I always seem to destroy everything, including myself.”16
“Some say I’m too sensitive, but the truth is I just feel too much. Every word, every action and every energy goes straight to my heart.“17
“It’s like always walking on eggshells” (being in intimate relationship with a BPD)18
Distinguishing BPD vs. NPD, BP, PTSD & ADHD
The following is a description of the similarities and differences between Borderline Personality Disorder (BPD) verses Narcissistic Personality Disorder (NPD), Bipolar Disorder (BD), Post Traumatic Personality Disorder (PTSD) and Attention Deficit Hyperactivity Disorder (ADHD). These diagnoses are often confused and sometimes can be co-occurring depending where the client is on the complex continuum of severity, sensitivity and external environmental influences. Also, as trauma has a profound relationship to affect dysregulation in the body, it is extremely helpful to understand how PTSD has some similarity in terms of how to treat BPD.
Narcissistic Personality Disorder (NPD) vs. BPD
Borderline Personality Disorder (BPD) can have traits of Narcissistic Personality Disorder (NPD). If BPD is considered as originating in early attachment, they both derive from the pre-verbal period of the first two years of an infant’s life. If not due to early attachment trauma, the traits may appear to be similar due to shock trauma. It can be difficult to determine BPD due to the often-overlapping aspects and the more common understanding of NPD. There also can be a co-occurrence with both disorders, in varying degrees.
According to Bioenergetic Character Structure, early developmental trauma of insecure attachment with NPD forms within the Oral stage of development, at an earlier stage than BPD, somewhere between 6 weeks and 1 year of age. BPD falls a bit later within 6–12 months of age. The Oral character is shaped primarily by the threat of abandonment. Neuroaffective development (the biological capacity for self-regulation) activates the core issues for all five Bioenergetic Character structures within the first 24–36 months of life19. This correlates with Schroeter’s theory (Schroeter, 2009) that aspects of BPD can be found within all Bioenergetic character types.20 See Table A below:

Table A: Bioenergetic Character Structure: Early Stages of Neuroaffective Development
Along with sharing common traits of shame, abandonment and rejection, NPD and BPD also share traits of conflictual relationships, low body feeling awareness, general anxiety, dissociation, and blaming. See list in Table 1 below:
Table 1 – BPD & NPD – Similar Traits
| BPD & NPD – SIMILAR TRAITS |
| Conflictual relationships |
| Low body feeling awareness Anxiety |
| Dissociation triggers |
| Blaming/projection |
| Core fear of abandonment |
| Shame, rejection |
However, there is a distinct difference in how they express their anger and handle conflict. A NPD person will often think that they do not need therapy. This is because it is difficult for them to actually feel their feelings in their body, due to missed cues from inadequate early bonding attachment with their primary caregivers. This causes core splitting off and dissociation within themselves. Blaming is a common characteristic where they will project the conflict that they create onto others. When their self-centred reality or what they want is denied, their anger often contains more critical and demeaning content. Refer to Table 2 below, regarding a list of differences between BPD & NPD.
Table 2 – BPD vs. NPD – Differences in Traits
| Borderline Personality Disorder – DIFFERENCES vs. | Narcissistic Personality Disorder – DIFFERENCES |
| Anger can be explosive, easily triggered – over-reactive or over-responsive (rage) to others (shame response to not feel rejection or abandonment) Anger can be unconsciously resentful, setting up conflict reactions in relationship (looping pattern is trying to unsuccessfully individuate) Anger can turn inwards, imploding, self-harm behaviours (cutting, suicidal) Anger can become chronic or suppressed into depression, despair or hopelessness (due to inability to tolerate intensity of core abandonment pain, shame and/or rejection) Feelings can switch quickly, dissociated from the other extreme Sometimes does not feel need for therapy (there is a continuum range) |
Anger is critical and often with demeaning content to self and others Great difficulty to feel own needs, their feelings with others, or for the feelings of others A difficulty to feel empathy or compassion for others (there is a continuum range of ability) Try to imitate feelings the best that they can (that they learn by observation), in order to get what they want from others Emotional range is narrow Often does not feel need for therapy (there is a continuum range) |
Narcissists have a continuum range of an inability to feel compassion or empathy for others. Because they are more disconnected from the feelings in their body, their consciousness cannot gather information to teach them how to imagine another person’s reality with the information of past experience of their own feeling affect states. Although they can appear to imitate feeling states to engage others to get their way, they are imitating actions that they have observed, to ensure they can control the relationship to meet only their own needs. Their greatest fear is of abandonment and it is unconscious – hence the inner reflection of abandonment is the actual dissociation from their body feeling states. It is normal for them to disconnect or not feel empathy for others, as they really don’t understand how that feels in the body. Life and being in the body is mainly a mental construct.
Both NPD and BPD individuals share a central fear of abandonment. In cases where there was abandonment and emotional needs not being met as infants, these individuals will project and act out various scenarios of abandonment dramas with others. In a narcissist, this plays out as a difficulty to be able to recognize or acknowledge the needs or feelings of others. However, BPD individuals are often emotionally highly sensitive and can be over-reactive or over-responsive to others in an effort to not feel their abandonment21 (including the feelings of shame and rejection that often go along with that). Anger may then begin to be felt due to some awareness of their own uncontrollable compulsion to constantly be aware of the other person’s needs first.
Over time, for some BPD individuals, this will slowly build up as resentment and they will unconsciously start to set up conflicts in intimate relationships in order to act out a need to feel separate from the other. (This is actually a healthy need to individuate that is unable to be resolved and has become distorted22) (Marahi, 2008).
Again, for some BPD individuals, their anger can go very quickly into a rage response. They are very sensitive and can be extremely easily triggered. However, they can also feel embarrassed or even remorse for their actions, but they won’t know how to stop or control this repetitive pattern of relating. For others, their anger can be suppressed and turned inwards into self harm behaviours (cutting), or depression due to a sense of hopelessness & despair at not being able to tolerate staying present to the core pain of abandonment, shame, disgust and/or rejection. They cannot change the ways they feel stuck in their unresolvable patterns.
Bipolar Disorder (BD) vs. BPD
BPD is also often confused with and misdiagnosed as Bipolar Disorder (BD). Occasionally it is co-occurring. They both share mood lability (poor affect regulation) and impulsivity, along with anger that is out of proportion to the current events, self-harming behaviours (high suicidal risk) and unstable relationships.
They also both have a tendency to think in extremes, such as you are all good or all bad. They have an inability to see people as having both good and bad within, as a complete concept of wholeness. You are one minute their closest friend and very quickly, you can become their enemy. There are varying degrees and levels in regards to how this trait of black and white thinking can manifest, but in general there is a strong tendency to not be able to hold two opposite extremes at the same time and consider a view point that is more generalized or complex. This may reflect their inner state as separate islands of consciousness that are not able to hold together as a cohesive sense of self within. Table 3, lists the common similarities of BPD & BD.
Table 3 – BPD & BD – Similar Traits
| BPD & BD – SIMILAR TRAITS |
| Poor Affect Regulation (mood swings/lability) |
| Impulsivity |
| Inappropriate anger |
| Self-harming anger, suicide risk |
| Unstable relationships Anxiety & depression |
| Black & white thinking |
A key difference between BPD & BD is that the Self-image of a BPD client is essentially bad and the self-image of a BD client is that of a grandiose (often arrogant) sense of self.
BPD has a more distinct reaction of a perception of hostility and autonomy (fear of separation/abandonment) in others then a BD client. The mood swings with a BPD client can be quite frequent from a few hours to a few days, whereas a BD client will have distinctly longer periods of time of mania/hypomania or depression. There are also reported cases of rapid cycling BD patients. The emotional reactions for a BPD individual may be triggered by a (perceived or real) fear of abandonment23, which is often deeply dissociated and may be the cause of an ongoing anxious state within.
A BD client will often not respond to a challenge or interpretation by a therapist whereas a BPD client will often have a strong emotional response – which can be expressed as anger/rage (somatic clues: increased agitation, hands clenching, foot tapping, increased tone {yelling}, become argumentative or defensive, etc.) or flight (somatic clues: eyes rolling away, head, foot or body turning to one side in an attempt to begin escape), dissociation (changing the topic immediately or ‘spacing out’), actually walking out of a session, or not coming back, etc.24.
Table 4 – BPD vs. BD – Differences in Traits
| Borderline Personality Disorder – DIFFERENCES vs. | Bipolar Disorder – DIFFERENCES |
| Self image is essentially bad (chronic shame) Mood swings from a few hours to a few days Interpersonal sensitivity to hostility and separateness A more distinct reaction of a perception of hostility and autonomy (fear of separation/abandonment) Often has a strong emotional response – which can be expressed as anger/rage = in constant relational conflicts Alternating idealization and devaluation of others |
Self image of a BD client is that of a grandiose (often arrogant) sense of self Long mood swings of several months usually with distinctly longer periods of time of mania or hypomania or depressions Interpersonal insensitivity Often does not respond to a challenge or interpretation by a therapist Uses avoidance and denial and may show poor insight |
Post Traumatic Stress Disorder (PTSD) vs. BPD
A primary concern for individuals with BPD is the difficulty in regulating the physical affect of their emotions. According to a study by Ford & Courtois (2014), BPD & PTSD overlap in 7 out of 9 DSM-V diagnostic criteria. General PTSD symptoms are often present in BPD due to a heightened sensitivity in the neurobiology of the brain and difficulty coping with traumatic external environmental stresses. They can both experience constant anxiety as well as the feelings of hopelessness/despair about their inability to regulate or control their emotional affect. This can cause chronic states of depression. This difficulty is due to the concept in trauma of the fight, flight and freeze response. In trauma, the body can dissociate from the intensity of painful and negative emotions in order to simply no longer feel them. This creates low body feeling awareness and many dissociation triggers that continuously loop. This chronic dissociative looping, based on emotional numbing, creates a sense of inner emptiness that both BPD & PTSD share as they feel stuck in a constant hopeless place of despair, with no capacity to understand how to shift out of it. The intensity is very difficult to tolerate and without adequate support or information about why this happens, they eventually can become a high suicidal risk. In adolescence, this risk for both BPD & PTSD individuals can be very high. However, often in middle age, the intensity of these symptoms can lessen, thus lowering the risk factors. Table 5 lists traits common to both25 (Ford et al, 2014).
Table 5 – BPD & PTSD – Similar Traits
| BPD & BD – SIMILAR TRAITS |
| Poor Affect Regulation (mood swings/lability) Self image is essentially poor (chronic shame) |
| Self-harming anger, suicide risk |
| Impulsive behaviour High anxiety Depression, despair or hopelessness Chronic Emptiness |
| Conflictual relationships (intense & volatile enmeshment) |
| Social detachment and avoidance Low body feeling awareness |
| Dissociation triggers Lack of ability to experience pleasure or positive emotions |
The essential difference between BPD & PTSD is that with BPD an extreme terror of abandonment or rejection as well as a strong tendency to alternate between idealization and devaluation of others is felt. This does not occur in PTSD or complex PTSD (cPTSD). It appears that BPD has a greater tendency to have both an under and over regulation of affect states, as well a tendency to have more under-affect when early childhood developmental trauma is confirmed. Under regulation means when someone expresses their emotional affect in a strong, perhaps over-charged, or highly dramatic expression. And conversely, over regulated is when emotional affect is more held back, more controlled or suppressed in some form. Complex PTSD has a tendency to exhibit complex combinations of both positive and negative dissociations with under-regulated affect states. Positive dissociative symptoms relate to active defensive responses and may include intrusive traumatic memories, flashbacks, intrusive voices, as well as complex patterns such as re-enactments. Negative dissociative symptoms relate to passive defensive responses and generally relate to loss of function which may include memory loss, higher cortical functions loss, loss of feeling, loss of motor control as well as loss of somatosensory perception (e. g. numbness)26. PTSD clients also have more difficulty recognizing emotions than BPD clients27.
BPD clients have different complex risk factors than PTSD that can be chronic and more dangerous to the self. They are also more likely to have co-morbidity traits with other disorders (such as Eating Disorders or Bi-Polar, etc.). They also appear to have a higher risk for re-traumatization in adulthood than PTSD clients. (Ford et al, 2014)
And finally, there is a small group of BPD clients that have co-occurring PTSD, as well as a small group of complex PTSD clients that have BPD as a subset grouping. There are distinct differences to be considered more in one category or the other. Table 6 lists traits that show the differences of both 28 (Ford et al, 2014).
Table 6 – BPD vs. PTSD – Differences Traits
| Borderline Personality Disorder – DIFFERENCES v. | Post Traumatic Stress Disorder- DIFFERENCES |
| Terror of abandonment or rejection Alternating idealization and devaluation of others More complex risk factors (than PTSD) that can be chronic, or more dangerous More likely to have multiple co-morbidity traits (<10%) that are more difficult to deal with (highest in Eating Disorders {50%} & Bipolar {35%}) Higher risk of re-victimization in adulthood due to those with early developmental trauma (A subset group of BPD patients may sometimes have PTSD as well) |
Complex combinations of both positive dissociation with under-regulated affect or negative dissociation with over-regulated affect (cPTSD) Has difficulties in experiencing and recognizing emotions Has both a varying ability to relate to beliefs within their own sense of self. (A combination of traumatic victimization and disrupted primary caregiver attachment relationships might be expected – BPD may be considered as a subset of cPTSD) |
Attention Deficit Hyperactivity Disorder (ADHD) & BPD
Although there are studies of a high incidence of individuals diagnosed with ADHD as children that are re-diagnosed as BPD as adults, there are definite differences. What is strongly similar is the poor ability to regulate their affect of emotional states and their impulsivity. ADHD could be an early childhood precursor symptom of adult diagnosed BPD. Table 7 lists traits common to both29(Ford et al, 2014).
Table 7 – BPD & ADHD– Similar Traits
| BPD & ADHD – SIMILAR TRAITS |
| Poor Affect Regulation (mood swings/lability) Impulsivity Conflictual relationships |
| Inappropriate anger Interpersonal deficits |
| High anxiety |
| Low body feeling awareness |
| Dissociation triggers |
BPD has traits that differ from ADHD in a few significant ways. There is a chronic feeling of emptiness that can be related to high-risk suicidality (along with shame, abandonment and/or rejection). There is a stronger tendency to dissociate. And although they both share a common trait of impulsivity, a BPD individual is driven by affective and interpersonal sensitivity aspects. ADHD is mainly about an inability to hold focus or attention, which is not a common characteristic of BPD. (While also similar for a PTSD individual, impulsivity for them is more related to deficits in attentional and cognitive processing due to behavioural inhibition problems.) There is also a tendency for some people with ADHD to always be moving in a constant hyperactive behavioural pattern. Table 8 lists trait differences between BPD and ADHD30 (Matthies et al, 2014).
Table 8 – BPD vs. ADHD – Differences Traits
| Borderline Personality Disorder – DIFFERENCES vs. | Attention Deficit Hyperactive Disorder- DIFFERENCES |
| A chronic feeling of emptiness Self harming behaviour and high suicidal risk A stronger possibility of a tendency to dissociate Impulsivity is primarily driven by affective and interpersonally sensitive aspects |
Inability to hold focus (loses attention easily) and/or high focus on specific areas of interest Tendency to be always moving (hyperactive) Behavioural disinhibition\Disorganization Responds well to medication Deficits in attentional and cognitive processing account for behavior inhibition problems, referred to as impulsivity |
Early Attachment & BPD
In the 1960’s, Mary Ainsworth identified these basic forms of attachment: Secure Attachment, Anxious-Avoidant Insecure Attachment, Anxious-Resistant Insecure Attachment/Anxious-Ambivalent Insecure Attachment. Mary Main, a colleague of Ainsworth, added a significant fourth category of attachment: Disorganized/Disoriented Insecure Attachment. This is the most dysfunctional category of insecure attachment styles. According to Main, disorganized attachment occurs when the attachment to the parent is frightening, frightened or dissociated and is seen as a ‘collapse’ strategy of the client who experiences ‘fright without a solution’ (Wallen, 2007)31.
Insecure attachment may develop with primary caregivers who have greater difficulties being fully present to their children for long periods of time during the first year of life, such as with: post partum depression, grieving a significant loss or terminal illness of a close family member (such as another child), experiencing severe relational stress with a partner (separation or divorce), a premature birth with incubation separation and/or a primary caregiver who may be in an accident or hospitalized. Adopted children may also develop insecure attachment due to separation from the biological mother and an unstable period of time with interim caregivers until an adopted primary caregiver is fully present in the baby’s life.
Mirroring: Peter Fonagy observed that secure attachment parenting was shown to be both ‘congruent’ and ‘marked’. This means that the parent’s facial and vocal displays correspond as an accurate and true reflection of their infant’s emotional expressions or affect states, rather than the parent’s state (Wallen, 2007)32. This became the basis of the child’s first representations of their own emotional affects, called contingent or emotionally attuned mirroring, which is the foundation for the infant to be able to self-regulate emotions as well as impulse control. According to Fonagy in a BPD client, the link is possibly severed or mostly disconnected within their consciousness between their internal experience and their reflection of responses from their external world environment (Wallen, 2007) 33.
When the mother is present to the infant, but not responding well to the infant’s experience it is called unmarked or non-contingent mirroring. Unmarked mirroring is when the baby can read the mother’s face for her responses, cues or distress signals and the mother (or primary caregiver) responds with her own needs, unable to give a coherent reflection that affirms a healthy response to the true needs of their child34. This unmarked mirroring is the core source of the developmental trauma form of BPD where there is an inability to be able to grow a secure attachment with the mother. This eventually translates as a non-cohesive sense of self that the child reasons as something that is ultimately bad or wrong within them, thus establishing a chronic shame and disgust based sense of self.
Non-contingent mirroring occurs when the child is invited to internalize the image of their mother/primary caregivers as their emotional self rather than be able to discover their own emotional self-state. This creates a vulnerability to a more narcissistic pathology and creates the split or illusion of a grandiose sense of self that swings back and forth with the empty sense of self35.
Understanding the non-verbal emotional affects of mirroring provides us with critical information in regards to how important it is to accurately mirror with words, tone, facial and body language through the relational treatment between therapist and BPD client.
Chronic Shame of the Borderline
The core issues of the early developmental trauma form of BPD is one of insecure or disorganized attachment. Either causes their sense of self to become unconsciously associated with the feelings of shame. Due to this early developmental trauma, they inherently believe they are bad. This also relates to their underlying intense fear of abandonment and/or rejection.
Chronic shame can also occur with other forms of BPD that may develop out of other external environmental stressors later on in a child’s life. The next direction of this paper is to follow how this relates to the experience of negative feeling states with the corresponding somatic affect states in the body. When we can track one form of BPD due to early developmental wounding, we can find clues as to how to heal or repair it later on in life through the integration of effective psychotherapeutic interventions, along with heightened body awareness of both positive and negative emotional affect states.
Shame (A Negative Affect State)
Shame is the hardest, densest energy band of consciousness to heal! It is so painful for most people that splitting off or dissociating from it is an understandable coping mechanism. This is similar to what occurs when trauma affects the body. To understand shame, we need to begin with understanding the physiology of negative affect states and how they represent themselves in the somatic expression of the body.
Tomkins describes shame as an indwelling affect that is inherent in the biology of the body (Helfaer, 2007)36. Through the pulsation of expansion and contraction, the body energetically shrinks back when positive connection is interrupted. A child can incorporate a chronic shame-system or self-hate system that is the result of the need to re-establish love (positive connection) and the child eventually becomes more shame vulnerable (Helfaer, 2007)37.
According to Donald L. Nathanson in his book Pride & Shame (1994)38, there are nine basic emotional affects (based on the seminal work of Silvan Tomkins39), through which our body instinctually expresses feelings. An affect is defined as the biological portion of emotion. When your face smiles, you are showing the affect of enjoyment. The circuitry to produce affects is stored in the primitive portion of the brain (brainstem) also called the reptile brain. When an affect is triggered it activates “a mechanism which then releases a known pattern of biological events”40. A feeling occurs when one becomes aware of an affect. Affects are an instinctual part of our bodies that we are all born with and express. From the minute we take our first breath we somehow know how to cry and scream for help or comfort. This occurs through a combination of the affects of fear, distress and perhaps also anger. Nathanson states that of the nine affects, there are two that are positive, one is neutral, and six that are classified as negative feelings. Next is a list of the nine basic innate affects from Nathanson’s book, Pride and Shame (some of them are listed as a continuum of a range of feeling)41:
POSITIVE
- Interest – Excitement (reaction to success/impulse to share) – smiling, lips wide and out, more charged energy
- Enjoyment – Joy (reaction to new situation/impulse to attend) – eyebrows down, eyes tracking, eyes looking, closer listening, the feeling of pride, more relaxing energy
NEUTRAL
- Startle – Surprise (reaction to sudden change/resets impulses, clears the mind) – eyebrows up, eyes blinking, hands may go up, body/head backwards
NEGATIVE
- Fear – Terror (reaction to danger/impulse to run or hide) – a frozen stare, a pale face, coldness, sweat, erect hair, eyes wide open, eyebrows up
- Distress – Anguish (reaction to loss/impulse to mourn) – crying, rhythmic sobbing, arched eyebrows, mouth lowered, an experience of deep grief
- Anger – Rage (reaction to threat/impulse to attack) – frowning, a clenched jaw, a red face, foot or hand tapping (irritation/agitation)
- Dis-smell [contempt/rejection] (reaction to bad smell/impulse to avoid – similar to disgust/distaste) – upper lip raised, head pulled back
- Disgust (reaction to bad taste/impulse to discard) – the lower lip raised and protruded, head forward and down, may have nauseous feeling in abdomen
- Shame – Humiliation (reaction to failure/impulse to review behaviour) – eyes lowered, the head down and averted, blushing
It is clear from this list that negative feelings far outweigh the positive 3:1. Shame is the hardest feeling to find and then to learn how to dissolve. Shame happens when the natural flow of either of the two positive affects, interest-excitement or enjoyment-joy, gets disrupted. Shame can limit empathy and intimacy by interrupting or interfering in consistent and safe connections with others. Quite often anger can be a response to the feeling of shame. This can be seen as a defensive response to not feel shame and an attempt to re-establish a positive feeling.
There are many other feelings, but Nathanson generally considers them as a combination of these basic nine affects. For example, he states that guilt is not a basic innate affect but an outcome of the combining of the innate affects of fear and shame together. Embarrassment & guilt are like shame, but they are about a behavioural response. Shame is actually a whole being concept, connected to one’s sense of self as being deficient.
The affect of Disgust can also be joined with the shame affect:
“Thoughts about being disgusting follow feelings of shame for several reasons. First it seems that the affect of disgust follows in the wake of disintegrating shame. Schore notes that in theories of development and psychotherapy, the affect of disgust is even more overlooked than shame. He cites a study that shows that persons diagnosed with borderline personality disorder or post-traumatic stress disorder (PTSD) – that is, persons suffering from severe developmental and relational trauma – are especially likely to have a disgust prone implicit self-concept. Disgust sensitivity is elevated in trauma-related disorders and this self-disgust is also likely to be dissociated.” (DeYoung, 2015)42
Shame is like a dark cloak, laid onto you by someone else. It occurs as a response from an external, outside source. It is a relational emotion that is about hiding from other’s projected judgments (perceived or real), harsh comments, criticisms or attacks.
Children are initially dependent on their parents to mirror their needs in positive responses or soothing, calming ways. When children experience a parent as raging or terrorizing in response to their needs, they will turn against their own positive life force, and eventually create an inner self that rages and is terrorizing against itself. This prevents healthy individuation and a great difficulty to honour or recognize their right to their own needs. This can also cause a constant experience of annihilation of their developing sense of self. Eventually they may repulse their own life energy – causing a self-hatred or disgusting sense of self43.
“Shame is an experience of one’s felt sense of self disintegrating in relation to a dysregulating other … someone close to us whose emotional responses leave us feeling fragmented …” – (DeYoung, 2015)
The affect of Shame is related to the sense of self. BPD clients truly feel like they are inadequate at their core as a basic human being. BPD creates a chronic core issue of shame and disgust about their sense of self. The following words embody the intensity of the shamed (with some disgust) sense of self-feeling states:
“Corrupted, Deficient, Not Good, Bad, Incomplete, Not Solid, Un-Definable, Un-Grounded, Un-certain, Un-worthy, Defective, Empty, Self-Hatred, Self-Damaged, Self-Sabotaging …”
Shame eventually can become an impediment to further positive affect. Over time, if one doesn’t feel enough positive affects (or positive neural pathway links that create positive affects), they can begin to lose access to them. This is what can happen if there are possible avoidant, ambivalent, resistant, disconnected or disorganized forms of insecure early attachment. These forms of developmental trauma set up complexities of emotional dysregulation. The negative feeling states, like shame and disgust then become difficult to stay present with. One can dissociate from these feeling states and it becomes unconscious. Any form of trauma can have a tendency to keep pulling one back, or trigger one into a negative feeling loop. It was either rarely or never experienced from early attachment with the mother what a good, safe, stable feeling state was or else it eventually becomes harder and harder to remember what it was like to feel good.
The somatic affect of embarrassment (a mild behavioural form of the affect of shame) can be seen at first as a slight flush, with red colour going up from the chest, through the neck and/or up in to the face. With the affect of shame, the head can subtly turn down and the eyes can be lowered, avoiding eye contact. Shame can also feel somatically like a large elastic band between two people that initially holds them together in relationship and then get’s dramatically and suddenly cut. The feeling as it snaps back to the person with the shame feeling is, “I must have done something bad or wrong to lose the connection”. It can be very fast and can feel like a strong slap in the face or like a push away in the centre of the body or like a prickly dread feeling of something dropping inside the body. Children unconsciously interpret this affect feeling state as if they must be wrong.
When children lose, or are unable to consistently hold a constant and loving sense of connection with a primary caregiver, it truly feels like the end of the world. It brings a sense of annihilation: a repeated feeling of death, over and over that becomes an integral part of their sense of self. This causes a non-cohesive sense of self that in turn creates a difficulty to effectively regulate their emotions. They can initially cry in reaction to the need to be connected (soothed, to feel safe and good again), however over time their system collapses and eventually the child gives up and dissociates to deal with this pain of dis-connection. This then eventually shifts into a chronic trigger of hopeless or despairing affect states and/or a looping anger state to protect and defend the self against the shame feeling state.
Healing Borderline Personality Disorder (BPD)
Working with integrated, somatic (body) based, psychotherapy methods can enhance the recovery healing work for BPD individuals. Discovering clues through the pre-verbal or non-verbal forms of expression during an infant’s awareness in the first two years of life can help guide practitioners in how to support BPD clients in reforming and reclaiming stable affect regulation, along with more consistent and stabilizing positive feeling states. This includes facial expressions, eye contact, tone of voice, sounds, touch, posture, intensity of contact, as well as pace or timing.
Next, are a few suggested approaches that can be applied to healing BPD through new relational entraining, developing a positive sense of self that holds, modulating affect dysregulation, increasing containment, developing healthy boundaries, integrating somatic experiencing trauma protocols and healing chronic shame.
1. Reclaim a positive core sense of self with relational, body focused psychotherapy (such as Bioenergetic Analysis). Working with developing or reforming the body and right brain connections, the mind can retrain its awareness into a stronger, more cohesive sense of self. New body experiences of positive affect states, containment and emotional management, become a doorway through the right brain processing, into understanding ones’ self as a positive and healthy individual. If there is early developmental or shock trauma, the therapist can support their client to grow and develop what is missing. Using body focused exercises, introducing new positive mirroring experiences, exploring the non-verbal, somatic attachment or relational issues allows the client to develop a new trusting and very real bond with their therapist. This in turn becomes integrated into a new relationship within themselves.
By learning methods that encourage positive body connections and cohesive emotional affect regulation, the client fills in the ‘holes’ that are missing in holding a healthy and consistent connection with their core self. A few ideas are presented here as introductory examples of how to work with developing a positive core sense of self through new somatic awareness techniques.
Understanding presence or being centred and grounded in the body needs to be developed. Presence is about embodying one’s conscious self fully present in the here and now. Trauma fragments the self and challenges the ability to be fully present in all aspects of one’s life. Worrying about the future (anxiety/fears) based on traumas of the past hinders the ability to live in the present moment. Being centred is about bringing one’s consciousness into balance within the body in the current reality. This can be done by developing a compassionate witness, by tracking sensory awareness of the various parts of self or how one organizes awareness of self through the head, heart or belly and in relationship to others44 (Maley, 2002).
Developing a consistent practice of body scanning to be more present in the body on a regular basis is achieved by teaching the client a new language to link their sense of self with basic body awareness sensations such as; heat, cold, tension, pressure, tingling, pulsation, pain (sharp, diffuse, shape, size?), etc. This can also be taught through touching the body, regular self-massage and/or naming the feelings and sensations to anchor them more consistently into conscious awareness. An easy accessible bioenergetic tool is to work with a rope, stick or various sizes and textures of small balls and use them for work with the soles of the feet to support more grounding ability.
Schroeter (2009), talks about the importance of understanding the difficulty to ground through the legs for BPD clients and to begin with emphasizing the feeling of safety through the relationship with the therapist first. The therapist’s body can be introduced as a new container for the self to safely and gently ground into, such as placing the feet or hands of the therapist on the client’s feet or placing their feet on the therapist’s belly/hips area. She describes the energy to either be split “between the upper and lower halves, with a tense midsection, or between the head and the body.”45 Schroeter suggests exercises that aid in developing positive, safe and grounding experiences in the body, such as holding the head and occiput area, as well as cradling the client’s body around the therapist’s back as they lie on their side, hugging the therapist with their whole body46.
Practicing daily mindful awareness of the body through grounding exercises strengthens connections of fragmented mind/body parts. It is important for a BPD client to regularly exercise the body to stretch it, stress it and feel the embodiment of its strength. Simple grounding exercises such as stretching and rotating all the joints, bending the back in 4 directions and twisting a stretch in the spine helps to bring back blood circulation, warmth, energy as well as more cohesiveness to the body and mind relationship.
In working with a large exercise ball, with the client and therapist sitting back to back on the ball, a client can grow into more connection and awareness of the spine47. Not only can one feel supported and ‘backed’ up, there is a corresponding sense of self that slowly begins to understand an experience of containment, connection, inner solidity or strength as well as gently encourage embodiment of their (missing or fragmented) parts. Bringing the spine back into relational awareness integrates the consciousness of the brain into the body more fully and supports greater connection to the core sense of self.
As the early insecure attachment form of BPD occurs somewhere in the 6–12 month stage of development, the back is learning to how to ‘stand up for itself’ as the baby transitions from crawling to standing. By focusing somatic relational work with the head, abdomen and spine areas, the therapist is able to integrate the split between the body and mind or the lower and upper half of the body through all the stages of attachment development. These forms of somatic interventions need to be repeatedly introduced in order to slowly entrain and hold the new conscious information into the body. They also should only be implemented with a body psychotherapist trained in the subtle and ethical awareness of touch in regards to early developmental relational work, trauma, sexual and/or cultural issues of body contact. Through new relational and somatic bonding experiences of safe, solid and positive physical contact with their therapist, the BPD client can develop a grounded and consistent, positive core self.
2. Understand Affect Regulation and develop new skills to modulate emotions. Affect regulation, the physiological expression of our emotions, are formed in the first couple of years of an infant’s life. Bioenergetic Therapists are trained to be able to coach clients how to manage under regulated expressions of emotions such as intense fear or explosive states of anger. Clients can be taught that by taking responsibility for their emotions, they can also learn how to re-direct them in safer and healthier ways. (Anger, for example, can be expressed safely through hitting a bed or pillows, or by lying down and kicking with both arms and/or legs.) There are many techniques that can be explored to manage and slow down intense emotional affects as well as strategies of how to manage feelings of overwhelm, high anxiety, anger or hyper-aroused states.
Bioenergetic Therapists can also help clients get more connected to over contained or over regulated emotions that may be more suppressed or dissociated. They can guide a client to discover what might be the deeper feelings underneath a particular intense feeling state or what may be the core cause of what is triggering them into negative feeling affect states.
It is critical for BPD clients to learn how to develop a range of healthy, positive, Resource Tools (see Item # 4 below for more about this) that help them calm down, contain and regulate intense negative affect states. This can be done through a variety of techniques such as (and not limited to):
- Practice subtle and deep breathing exercises to calm and slow down both body and mind. Due to the split or contraction in the mid-section of the body, the diaphragm of BPD clients will be more constricted and tight48. Most BPD individuals will breathe more in the upper chest area, unable to contain their feelings more fully into their body and thus are under-regulated in their emotions. Practice breathing exercises such as counting as you breathe out (exhale for longer to expel more air) by counting to 5 or 7 slowly before breathing in. This slows the breath by forcing longer and thus deeper in-breaths through the diaphragmatic block and into the lower belly.
- Release deeply held tensions and trauma in the body through simple exercises that encourage deep spontaneous trembling. A good resource of one form of a Bioenergetic based practice are the Trauma Release Exercises (TRE) by David Berceli49.
- Include a Dialectical Behaviour Therapy (DBT) approach. DBT is a more structural (left brain) approach that advocates client commitment and the ability to self-monitor and track on the part of the client. It includes a dialectical approach (a synthesis of opposites, non-absolutes, fluidity of change), mindfulness practices, new skills training and consistent follow through50. DBT helps clients become aware of and track triggers that cause emotional dysregulation, as well as tracking how effective their newly learned skills and coping strategies are working, which provides hope out of their despair state. This type of individual therapy, integrated with group therapy, works well as it connects the mind and body.
- Express feelings through right brain explorations of movement, sounds and creativity. Forms of dance that encourage spontaneous, intuitive or authentic movement allow the body healthy forms to express difficult emotional states. Drawing emotional states with intuitive, abstract expressions of colour and shape can move negative emotional energy through the arms, hands and out of the body. These drawings can also be interpreted afterwards, similar to interpreting dreams, to access the unconscious meanings. Spontaneous sounds, chanting or singing can also move distressing energy through the body and shift it into more positive or calming energy states.
-
Experiment with various forms of Energy Psychology. Many forms of Energy Psychology follow Traditional Chinese Medicine (TCM) awareness of energy meridians throughout the body and supports triggered sensitive systems that get easily overwhelmed51.
- Learn Emotional Freedom Technique (EFT) tapping exercises (again, based on TCM awareness of shifting energy), which help reprogram the brain and body connection of intense negative emotions and belief systems52.
- Practicing Donna Eden’s Energy Medicine exercises such as the 5 Minute Energy Balancing routine, or the Triple Warmer calming method helps to calm hyperarousal found in PTSD or BPD.53 54
- Explore Structured Therapy for Affective and Interpersonal Regulation with Modified Prolonged Exposure (STAIR-MPE)55 or Trauma Affect Regulation: Guide for Education and Therapy (TARGET).56
3. Containment Work. An important aspect of healing the core of BPD is strengthening and building new connections for a more contained and boundaried sense of self. Learning mindfulness techniques strengthens the mind to stay with the present moment and let go of future worrying or constant, unfocussed thinking patterns. It is helpful to join a meditation centre, take courses and/or go on regular silent retreats to develop these skills with others present, as group energies can support entrainment of new neurobiology patterns in the brain.
Journal writing is also a great form to track, explore and re-write one’s personal narrative of how BPD individuals can view themselves. It helps to hold the memory of the split off parts as well as encourages self-reflection, problem solving or decision-making. It also offers opportunities to re-write the stories with new information, as one understands oneself on increasingly deeper and more integrated levels.
Anger and boundary work can often be important ways to help re-claim the body. For many people the affect of anger needs to be re-organized to support the self to get what it needs, rather than be turned inwards as self-harm or outwards in ways that can be sabotaging of intimate or work relationships. With early developmental trauma, anger can sometimes be a very difficult feeling to actually connect to and feel. Trauma may also cut off the feeling of anger or shame due to the freeze response of dissociation needed to separate from the pain of the event/s.
Boundaries need to be taught with an emphasis of how to actually feel them with the body. Although traditional talk therapy can be very helpful in creating a clearer narrative about who one is, working with the body can often make faster significant shifts that translate well into new modes of functioning in the outside world. Standing exercises with a string placed in a circle on the floor around the client (that they place) and walking towards them slowly (on all 4 sides of their body) can demonstrate how they respond (by neutrally observing breath, micro movements, facial expressions, sense of pressure, etc.), begins to teach a simple awareness of an energy boundary around their body. Or playing with pushing with their hands with the therapist (also while standing) and expressing push and pull movements with verbal expressions of ‘No’, “Go away” and/or “Come here” emulates the rapprochement stage of attachment and can teach new body/mind connections of a client’s actual needs. Boundary work can also be explored on a number of other levels such as in intimate or professional relationships, learning how to write clear contracts with others, or perhaps in developing the discipline to organize and maintain an ordered lifestyle and physical environment.
Shapiro’s work with Bioenergetic exercises of curling and uncurling the body through charging and containing can be extremely helpful for BPD clients. Developed as a gentle approach to help restore natural energetic pulsation, Shapiro’s exercises provide containment for building boundaries through somatic experiences. Some of these exercises help to calm the system and others can charge the system (Shapiro, 2008) 57. Shapiro’s seminal guide, ‘Bioenergeric Boundary-Building’ contain an extremely helpful series of exercises that may also be explored (Shapiro, 2006)58.
Exploring solo journeys in Nature can offer experiences of more self-reliance skills that can create space for a healthy individuation of the sense of self to develop. BPD individuals may have a general tendency to merge too much with others and rely on them to initiate events or make decisions. Independent, solo explorations include simple mindful walks in the park, biking on remote nature trails, solo canoe or kayaking day trips. Eventually one can go on longer wilderness, canoe or hiking trips to challenge themselves and experience successful adventures of independence on their own.
Finally, it is often useful in containment and boundary work to develop a personal connection with a form of spirituality that can transmute confused or negative attachments to a constant, loving, compassionate form of attachment. For example, shifting the experience of a negative mother to a positive form of “Divine Mother” can be extremely helpful and freeing.
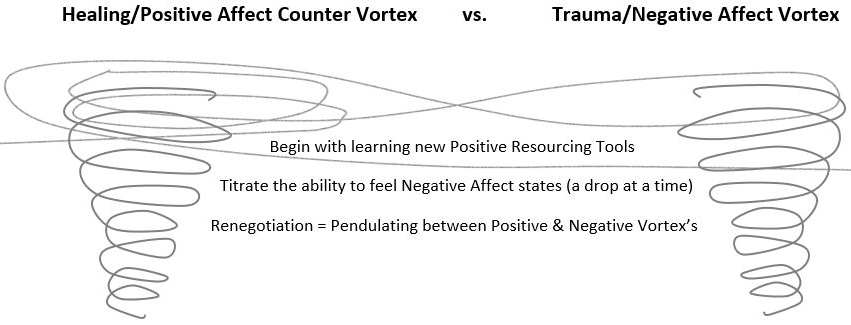
4. Work Slowly with Somatic Experiencing Trauma Protocols: Resourcing, Titration, Renegotiation, Healing/Positive Affect Counter Vortex versus Trauma/Negative Affect Vortex (This section is largely based on the work of Peter Levine59)
Resourcing: It is important to be able to re-organize the meaning of what it is like to be in the body in order to feel and heal negative affect states. Body sensations, fear, anger, shame, abandonment and/or rejection are often hooked together in trauma or early developmental injuries. To uncouple these negative relationships, the idea is to initially learn body awareness of experiences of pleasure and safety. The client needs to learn from scratch how to be able to contain, regulate or negotiate the intensity of their negative emotions. This will eventually give them some measure of control and safety to be able to come out of the negative sensorial feeling states in the body, on their own. Levine calls this Resourcing (1997) and there are a great variety of tools that one can implement to achieve and reconnect to positive affect states60.
As trauma often causes PTSD symptoms, the body can get stuck in one or a few negative affect states. Anger or shame are often experienced as negative or bad, uncomfortable feelings. The experience of feeling overwhelmed or flooded by too much (intense) feeling is part of the fear affect response. With trauma, fear creates a fight, flight or freeze reaction. In the freeze, there is numbing (being present to the trauma, but unable to move or respond in fight or flight) or dissociation (when the consciousness leaves the body and there is no memory of the event). This is an instinctual protection mechanism that is dealing with the trauma of an event.
When the body is stuck in the frozen state, coming back can be enabled by slowly going through the physical actions of the flight or fight motions in the body. This gets the energy unstuck and moving through again. Individuals can be stuck for years with the affect state energy patterns frozen in an actual twisting in their spine or torso, or body part tremor, or a kind of numbness or deadness in a body part, etc. With trauma, and with shame, the fear aspect of it causes a part of the self to leave the consciousness of the body. This is also what causes the intense emotional pain or discomfort that can trigger self-harming (Page number)behavior actions where anger comes through to try to create change and hits a block, or the stuck place in the trapped, traumatized energy and attacks the self instead, expressed as self-cutting or possibly even suicide.
In a trauma body, body sensations may initially be interpreted as negative sensations. The experience of feeling overwhelmed or flooded is a fear response. It is not pleasant to go into the body if it is in fear. Learning how to visualize and experience good feelings in the body becomes the initial focus of reclaiming the body mind emotional regulation work. Positive Resources can be used to create new systems to help self-soothe and regulate the overwhelmed nature of a trauma system. In this light, addictions (such as alcohol, smoking, drugs, food, etc.) can also be seen as a way to help regulate the affect of high anxiety and help to self-soothe. If a therapist is working with a client with any form of trauma, to remove an addiction prematurely before other resources are able to be introduced, integrated and effective, rarely works.
For a BPD client, once the level of a self harming threat crises is safely mitigated, the main goal is to teach self-soothing techniques to help calm the dysregulation of their emotional affects. BPD individuals are highly sensitive and constantly easily triggered. Teaching them that they do not need to feel like victims that cannot control their emotional liability, empowers them. Through learning with a variety of new relational experiences and different forms of exercises that they can practice on their own to manage intense emotional feeling states, gives them hope. They also can gain a greater understanding of what they can do to disrupt the negative feeling state in their system, with increasing speed.
Titration: Re-organization: Positive Resourcing needs to be learned slowly and takes time as any feeling (positive or negative) produces a charge of energy in the body and thereby creates more oxygen and life in the body. More feelings can activate an overwhelming response that floods the system causing panic, numbing or dissociation very easily.
Titration, another term borrowed from Levine61, is standard practice in this kind of work. Allowing a drop at a time to enter the system, can slowly and gently re-organize the original experience to integrate safety into the body. As Jacqueline Carleton states, “… pausing in the account to allow the nervous system to – recycle, avoids iatrogenic re-traumatization. This can be done in a number of ways: by resourcing at the beginning and as it unfolds, by asking the patient to focus in the present, and by any one of a number of grounding and stabilizing exercises”62 (Carlton, 2009).
Establishing new resources of information that encourages body and mind to connect to feeling states of safety, pleasure and connection are the next steps. Learning how to calm the body down quickly, when triggered into a fear, angry or a hopeless/despair state, is essential in understanding how to regulate the affect states of intense emotions.
Renegotiation: The Healing/Positive Affect Counter Vortex vs. The Trauma/Negative Affect Vortex63: With heightened sensitivity to negative emotional states in a BPD individual, often something will be triggered that overwhelms the system and it can feel like one is falling backwards into some or all of the ‘old’ (from the past) feelings of: negativity, despair, hopelessness, annihilation, self-abuse/sabotage, rejection, exhaustion, collapse, and/or contraction. It may continuously feel like the past trauma or disruption of positive feeling stability intrudes onto the present reality. Working with a Healing/Positive Affect Vortex concept, includes having a number of different resourcing tools to counter-balance the Trauma/Negative Affect Vortex (Levine, 1994) experience.
Once the body begins to learn to feel safe and has had some experience of calm or pleasure, one can then begin to allow some of the more intense, negative feeling states to enter the therapy and become re-organized. This is a process called Renegotiation (Levine, 1994), and is the core work of how to introduce emotional regulation back into a dysregulated system.
To pendulate between the Trauma/Negative Affect Vortex and the Healing/Positive Affect Counter Vortex (Levine, 1994), allows for a slowly increasing ability to contain and transform the triggers and disruptions of the body mind relationships into new, positive experiences in the body.
Introducing humour and more playful approaches to connecting with the body can also be extremely helpful in transforming, reducing or shifting the negative affect states, including flight, fright or freezing responses that may occur when trying to integrate consciousness and emotions. This slowly grows an ability to modulate affect regulation more gently with the body.
5. Healing Chronic Shame. Self-acceptance and self-respect are the antidotes to shame. Through acceptance of the flawed, negative self (that includes shame, disgust, and/or hatred), we develop a form of self-respect that allows us to suffer these feelings, “rather than suffer the effects of the struggle against them” (Helfaer, 2007)64. Helfaer emphasizes the importance of understanding how the poles of the idealized/self-denigrated self can get played out in the dialectic of narcissism through the need to be seen as special (positive pole), or else as worthless (negative pole) (Helfaer, 2007)65. Self-respect is developed through the healthy integration of the positive and negative self.
Explore with the client their shameful as well as courageous and prideful stories. Supporting a BPD client to claim a narrative of their past shame helps to link and reconnect the dissociated parts of themselves into a cohesive whole. This needs to be done by a therapist whom they have developed trust and bonded with. Using the above trauma protocols of titrating positive resources into the body’s somatic shame reaction slowly dissolves the hidden holes (or blocks) that shame creates in the core sense of self for BPD clients.
Following the shame narrative with stories of courage and pride, the therapist can often reframe the shame story segments through loving acceptance or being non-judgmental and filling up the neural networks in the brain with positive feeling states. Exposing the shame story of a BPD client, with the essential somatic and relational mirroring of the compassionate and caring eyes of a therapist ‘seeing’ them as they talk about it, can gently transform their chronic shame self into a more joyful and proud awareness of self.
When a client shares their shame and pride stories in a larger group setting, this allows the community to also ‘see’ them with compassion, in a larger collective reflection. Hearing the shame and pride stories of others in a group setting, can offer other clues to the dissociated, fragmented parts that may be missing in a BPD client, due to the way shame is so often lost and hidden to the self. This kind of group work reclaims missing parts and has the potential to transform shame at deeper levels.
In addition, although it is not in the general scope of psychotherapy, the somatic psychotherapist is interested in helping the client live a balanced life. As an adjunct to therapy it can be valuable to recommend support from the adjunctive fields of healthy eating or natural remedies. Many BPD individuals are highly sensitive or intolerant to sugar and/or other foods. Practicing a healthy diet and possible work with natural remedies can support a more balanced emotional regulation and aid their healing process. Also, with the heightened sensitivity of BPD individuals, they will likely be very affected by electrical and electromagnetic energies and alcohol or other drugs as well. This may constantly destabilize their energy into negative feeling states and scramble the energies of the body and mind causing a greater inability to focus or think clearly.66
Therapist Somatic Counter-Transference with BPD
For the body-oriented therapist, there are many opportunities to be aware of counter-transference or somatic counter-transference issues when working with BPD clients.
In general, counter-transference issues with many clients as well as BPD clients, can include the following in regards to the difficulty to holding boundaries:67
- A therapist can get drawn into more intimate physical or sexual behaviour due to the blurring of clear ethical boundaries.
- The therapist may offer inappropriate self-disclosure and not be able to hold a “personal information” boundary for him or herself.
- Ethical transgressions can occur with a sense of over responsibility for the client, trying to rescue and problem solve for the client (rather than encourage them to solve their own issues).
With BPD clients, there are a few more possible transference issues:68
- The therapist can get pulled in, loosening their professional boundaries and become too involved with their BPD client.
- The therapist can be manipulated to give the BPD client special considerations because they are seen as special and in order to ward off the client’s angry responses.
The therapist can begin to develop loose boundaries by extending a session, allowing extra or excessive phone, text or email connection between sessions, deferring payment, or not charging a fee. It can be a complex process for a therapist to be clear about what is theirs and what belongs to the client. While this is generally true, it can occur more often with BPD’s because of their own lack of clarity with personal boundaries. Depending on the severity of the wounding, a professional therapist may need extra support working on counter-transference in supervision or seek back up support within a clinical setting, their own therapy and/or group supervision.
A significant counter-transference issue can occur when a psychotherapist experiences alternating feelings of fear, anger or helplessness/hopelessness/despair that exists within the BPD client but is dissociated from their awareness. This can be experienced somatically in the body of the therapist during, as well as between sessions69. To be able to respond effectively with a BPD client it is important for the therapist to become aware of their own personal history of helplessness or anger and get clear on how those feeling states can manifest somatically in their current body physiology or be acted out.
“They [BPD clients] can provoke feelings of helplessness and anger in service providers. It is, therefore, vital to set and enforce limits so that the treatment provider can remain involved, compassionate, reliable, and consistent (Oldham, 1990, p. 306). Sperry (1995, pp. 65–66) noted five points of consensus in treating individuals with BPD:
– the service provider must be active in identifying, confronting, and directing client behaviors;
– there must be a stable treatment environment;
– BPD clients must learn to connect actions and feelings;
– self-destructive behavior must be made ungratifying;
– and countertransference feelings must receive careful attention.”70
The triggering of the counter-transference of anger within the therapist is a challenging affect to work with. The client may create little set-up games without being conscious of it inspiring conflict. This has two possible directions. One is a natural desire to individuate. The other is about creating more focus and intensity so as to hold connection and be more present in the body, rather than disconnecting. To work with this, it is important to hold your own centre and simply not react. To start with you can lower the tension by agreeing quickly with the client’s different point of view to diffuse the conflictual energy being presented.
The best way to work with the alternating states of anger and helplessness (or hopelessness/despair) is to gently begin to name the feeling state in your body and ask the client if they have any sense of this state in their body. It is important to do this repeatedly as they will likely be disconnected or dissociated from the ability to feel this state at first. Be prepared for denial initially and do not let it stall you. Regarding the helplessness state, to simply name it when it shows up and not show your own fear, or be overwhelmed with panic or hopelessness of the ‘stuck’ state. It is important to be able, like the mother or caregiver, to “mark” body-sensation and feeling with accurate mirroring reflections through voice, tone and body language affects. This will allow them to eventually simply be present to that state within themselves without judging themselves into a defensive or dissociated shame response. Then you work with inviting gentle self-soothing techniques to feel safety and pleasure again to bring them back to a positive feeling state within the body.
A BPD client can create, within their therapist “… a maelstrom of deadness, emptiness, despair, and terror with no exit”71 (Baum, 2007). Scott Baum talks about the concept of ‘Soul Murder’, as a direct effect of terror in the body that a BPD client may experience from the early developmental form of relational trauma. He describes it as a direct experience of annihilation that is like a ‘living death’ within. Baum feels that it is critical for the therapist to be able to stay present to these terrible and intense negative states (also including helplessness, abandonment, rejection, shame, disgust, hatred, etc.) (Baum, 2007). It is important to be able to name and validate these negative affects and affirm the real truth of the agony of experiencing them. This allows the client a new opportunity to learn how to be able to emerge through them into a positive connection of self and other, through the transformational, healing relationship with their therapist.
The following is list of various feeling states that can be experienced somatically by a therapist as a potential counter-transference issue with a Borderline client. It is important to be very familiar with what these various feeling states feel like in the therapist’s body, so that when they are experienced while being present with the client, the therapist can note his or her somatic states to gain clues as to the feeling states going on with the client. These clues can be explored by the therapist as to their counter-transference possibilities by knowing and owning their (the therapist’s) own personal somatic states of emotional affect. Supervision with a body-oriented or Bioenergetic therapist can greatly assist this process.
Anger
BPD clients may often experience anger and aggression and may also at times deny their own sabotaging or angry state and set up a dynamic of triggering others into acting out their anger. They can also continuously get triggered into a shame response, and may deflect to anger, as a secondary emotion, in order to protect and defend the vulnerability of feeling badly about themselves. They can be very destructive and their anger can get out of control with little affect regulation to moderate certain situations if needed. Their general aggression can be interpreted as a chronic and unconscious underlying rage at the absence, abandonment and/or rejection of a parent who was the primary caregiver.
As a secondary emotion, hidden underneath anger, there may be deep emotional pain such as grief, fear or shame. Anger can also co-exist with one or more of these secondary emotions. Sometimes this is possible, but this also makes it confusing to sort out what is really going on as the core reason of why there is anger, and what the message of anger could be trying to express in the client. The body is trying to achieve balance in some form. Anger can sometimes be understood as information from the body of a need that is not clearly identified.
Anger usually comes up because we are not getting what we want. We want something to change in order to be released from a negative emotional discomfort in our bodies. Anger can make things happen. It can be an instrument of change with an expenditure of energy. Some people learn that with anger, there is a force that can push through to get them what they want.
Teaching self-reflection can start the process of loosening the block that the message of anger is creating inside the body. To help a client possible questions to ask are:
What am I holding back?
What am I holding on to?
What am I needing here?
What am I not getting?
What am I afraid of?
What am I not wanting to feel or see?
What (feeling or thing) might I be hiding from?
To manage somatic counter-transference it is helpful to be able to read the unconscious expressions of anger that the body will exhibit. Concentrating solely on the affect of anger, its expression in the body can be seen through the basic tensing and contraction of tissue and muscles. There are multiple variations of this such as the face going red (skin tissue inflamed, contracted), a frown (mouth muscles turning down, contracted), yelling (throat muscles tensing), and/or swinging out with the arms to hit (arm and hand muscles tensing and contracting).
One can also hide, repress, or suppress an angry affect in a number of ways. Some ways to hide anger are tensing your shoulders, clenching your jaw, clenching your fist or knuckles, tapping your foot, or feeling restless.
Irritable bowel symptoms can be the result of tension in the intestines related to feelings of fear and resentment (holding onto anger)72. Traditional Chinese Medicine (TCM) suggests that liver issues may be created by an imbalance of anger and gall bladder issues may involve deep resentment or holding onto anger73. Skin irritations (eczema), muscle inflammation, or arthritis may all be expressions of somatised anger or rage in the system. In these ways anger can be somatized in the body without the mind having awareness of any anger.
It is also helpful to establish a secure bonding of trust with a BPD client and build positive resources of re-connection before getting into challenging the defensive strategy of continual anger looping. To begin to untangle the complexity of their negative emotional states, be aware that their anger defense allowed them to survive up to the point of therapy. It may also be helpful to explain to them that this anger is trying to protect them from what happened in the past, but now it is time to let it go, and to transform and re-organize their anger to be more effective in their current life.
It is critical to understand how to work with the high sensitivity aspect of a BPD client. Do you find yourself feeling afraid that you may trigger your client in an angry or rage state at the slightest thing? Try to not get defensive. Pull back, do some subtle breathing exercise work during the session to come back to your own body presence. Focus on reflecting back their angry affect state without judgment in either your facial expression or voice tone. Show concern and repeat their words back to them or explain their body action of their anger affect state. Help them make the link between the observed state and what they are actually trying to ask for in the anger reaction. Be consistent and clear about your limits, what you need to be safe and follow through with holding your boundaries. They need to feel these limits to feel safe themselves.
Abandonment
Clients may miss appointments or find it difficult to stay present or focused during the session. Do you notice them pausing, freezing or tuning out for a few seconds while they speak? This is a sign of dissociation, which can also be seen as an act of abandonment from themselves. It is a reflection that what was done to them in the past is occurring within them now.
The somatic expression of abandonment is a sense of disconnection from the sense of self. It feels extremely isolating and alone. You, (or your client) could feel “spacey” (in a dreamy state) or not grounded in your sense of self or in the body. Or you could feel nothing somatically in your body at all, which is often a strong sign of dissociation in the client. Anger can also be a response to abandonment. However, in early developmental trauma, the child’s anger may have received no response, in which case it becomes dissociated in the adult client and thus more likely to be felt in the body of the therapist.
Check in and ask yourself if you feel irritated by their abandonment, dissociation or denial of their issues? Are you aware of feeling the client’s dissociated anger (from being abandoned)? Or do you feel nothing or feel like you are alone in the session with your client, perhaps trying too hard to get them to do anything? If so, you may be in the presence of a client in a fragmented, abandoned state.
Annihilation
Annihilation feels like either the person you are, or your point of view doesn’t exist. It feels like you are unseen, unheard or invisible. The client can feel like a ghost inside an invisible body. It is such an intolerable and terrifying feeling that most people dissociate from it.
Annihilation has similar somatic states as abandonment with essentially no feeling in the body at all. As the therapist, do you feel like you don’t exist to the client, or that your work/influence appears to have little or no impact on the client’s progress? If so, you may be in the presence of a client experiencing an annihilation state.
Bewilderment/Confusion
Bewilderment is about feeling lost or confused as to what to feel or what is going on. The feeling of confusion can be induced by constant overwhelm or too many feeling states. It can be experienced as a kind of shock state. You (or the client) may feel spacey. The client’s eyes may be open wider in a surprise/startle state. Or they may move around a lot trying to understand something beyond their grasp. The body can also feel numb or nothing at all – it can dissociate from too many confusing and varying feeling states.
In this case are you, as the therapist, aware of nothing in your body while with the client? Or do you feel stuck, bewildered or confused yourself while with the client? Does your client make you feel a little crazy (switching to many different emotional states constantly and so quickly)? If so, you may be in the presence of a client in a bewildered/confused state.
Despair/Helplessness/Hopelessness
You may find yourself at a loss as to what to do or how to respond to your client when they are in a stuck or helpless state. The ability to stay present with a BPD in the intense feelings of hopelessness and despair can be very challenging for most people.
Maybe you feel like giving up working with this client? Or do you feel that you don’t know how to help them anymore? If so you may be in the presence of a client in a despair/helpless/hopeless state.
Are you familiar with or able to stay present to your own inner place of despair/helplessness/hopelessness? Have you made peace with or do you have an awareness of acceptance of this place as a part of yourself and the human condition? Are you able to sit with others with acceptance, compassion and/or space for this feeling state? Personal therapy for the therapist to explore this challenging and intense negative affect state, may be helpful to support this deep level of work with others.
Disgust
The affect of disgust comes up deep from the belly and it can feel a little nauseous or like you are about to throw up. The mouth can go into a frowning, pucker shape, with the tongue out a little, mimicking a regurgitation reflex. And the nose can wrinkle up slightly as if smelling something bad. Disgust is mostly about disliking or hating the core of the sense-of-self.
Perhaps you don’t like your client, or maybe you really hate working with them? Or you may just know that you feel better than this client. Do you feel superior to the client? Does something about the client repel you? If so you are likely in the presence of a client in his or her own disgust state.
Fear/Overwhelm/Terror
The affect of fear has a continuum of expression from slight overwhelm, to mild anxiety, to occasional panic attacks, to various fears and phobias, to extreme terror. Fear causes the energy in the body to retreat from the periphery to focus into the core of the body, surrounding the organs and viscera in the centre of the body. An image of a full fear state is the body being in a contracted fetal position, lying down, curled up on one side. Both the body and sense-of-self contracts. Before this state, the body goes into the fight, flight or freeze mode. In full contraction, the body is in a freeze state and can then dissociate from the feeling states.
Terror is a more intense feeling of fear, one of falling apart and losing control. This can cause complete emotional dysregulation.
Again, use your body’s somatic awareness for clues about the client’s state. Is there dissociated fear or perhaps a stiffness or tightness in your body or in the client’s body as you observe them? It can sometimes feel overwhelming to be with a BPD client because their intense affect states or constant swings in mood liability can be challenging for most people. Do you feel like screaming inside when with them or can you sense their inner scream of fear/terror? If so, you are likely in the presence of a client in a fear, overwhelm or terror state.
Self-Sabotage
Self-sabotage occurs as a form of unconscious anger that clients act out, which is ultimately harming to them. Self-sabotage is when the energy of anger implodes and get’s directed inwards (part of a shame response) and unknowingly, eventually harms or destroys something for the client. It happens when anger gets distorted or suppressed and does not work in a constructive way to help them get what they need. Self-sabotage is more about how the client’s actions are harmful to themselves, rather than as a somatic expression. However, self-harming behaviours such as self-cutting are a somatic form of harm to the body where the anger implodes and gets inwardly directed.
Can you catch if you are feeling angry with yourself for doing something wrong with your client? Or perhaps you let slip an irritation or judgmental remark with them? Or maybe you made a mistake with them because you may have been overwhelmed by their intense anger or fears. If so, you may be mirroring your client in a self-sabotaging state.
Rage
Rage is different than anger. Underneath rage is helplessness. If it gets fully expressed, body feelings can become completely dysregulated. Rage can also be about terror. It is a reflection of survival from a very primal place. The somatic expression of rage is a scream that comes through the whole body. To support clients in expressing this rage, allows them to be contained by your presence so that they can fall apart to let the scream through and find a place of peace afterwards by letting this out of the body.
Can you sense a scream inside your client’s body? Do you as the therapist have a desire to scream when you are with your client? Does your client make you feel so distressed sometimes that you want to scream? If so then you are likely with a client struggling with a dissociated rage state.
Rejection
The somatic experience of rejection is very intense and most people do not want to feel this negative affect state. A client might feel like they cannot breathe or that they are suffocating. They can feel like their heart is split in half or fragmented in a million pieces or that their body is crumbling and all the muscles are going into spasms. It can feel like a sharp jabbing, knife like pain, or like a sharp slap in the face.
Do you find yourself being judgmental, or feeling contempt? Do you find yourself accidentally making your client feel bad or wrong during a session? Are you aware of your own story or feelings of rejection in your somatic history awareness? Your client may be in a state of acute or chronic rejection, possibly co-occurring with shame and/or abandonment states as well.
Shame
As stated earlier, the somatic effect of shame can be seen with the head subtly turned down, eyes lowered, or eye contact avoided.
Are you making embarrassing mistakes, or do you feel that you cannot ever get it right with your client? It can be challenging to connect with the feeling of shame in the therapist’s somatic counter-transference. If you are familiar with the somatic states with your own shame story, it will be easier to identify what you are experiencing when working with the client. The shame is either yours or may belong to the client who is in a dissociated shame state.
Summary of Clinical Counter-transference Issues
For psychotherapists, it can be very supportive to use a more body-focused approach when working with BPD clients. Self-regulation can be taught through body sensation awareness to link the feelings to the physiological expressions of the emotions, then to their conscious thought patterns. Non-verbal cues can be significant entryways to hearing what the body is actually trying to express in somatic trauma patterns. It is also important to let clients lead with their ability to stay present to the work (not dissociate) and handle the degree of slow body sensation awareness recovery work. It is supportive for the therapist to take the time to understand attachment neurobiology and how bonding can be reformed through eye contact, presence, authentic mirroring of the client’s self, the sense of safety, loving gentle touch and/or respectful body contact affect regulation work. Repair through somatic resynchronization is possible and re-establishes basic trust, emotional regulation and a healthy maturation of self74 (Bentzen, 2015).
Healing a dysregulated system requires the ability to learn how to trust that by letting clients go into intense negative feeling states, they will naturally be able to come back into a more regulated state. They can become deeply dysregulated (e. g. have flashbacks, fall apart), however through gaining positive resourcing skills that clients have practised, they learn safety and how to trust that they know they can come back again to a place of coherent regulation. This allows them to slowly build up a stronger containment of their sense of self into a new, integrated whole that includes and slowly transforms the intensity of dysregulation of their negative feeling states.
The authentic and direct relationship with the psychotherapist is also an important component of healing a disrupted early attachment bonding with BPD clients. It may be helpful for the practitioner to educate their client by introducing ideas of how conflict can sometimes be an opportunity to repair the disruption or disconnection looping of the past and grow into a more consistent and permanent connection with their self in the present. Learning how to repair the trust that was lost with the ‘other’ and regain it back within their self is a significant step to building new neural pathway bridges in the brain, which translates as a stronger, more solid and contained sense of self. Learning to not lose themselves in the disconnection cycle, but to know that they can continuously repair and come back, over and over, is an important and significant new experience they can grow into within the relational aspect of the work with their therapist.
It is important to find therapeutic support that includes some somatic affect regulation training and/or some trauma PTSD awareness.75 This work can also slowly shift the self-shaming shadow and stigma that often permeates BDP clients by not seeing their issues as isolating, and alone, or their fault, thus allowing them to change a chronic experience of powerlessness or victimization into one of growing empowerment.
Summary
This paper summarized how Borderline Personality Disorder is defined as well as described some unique features of how it is experienced. It compared the sometimes complex and co-occurring traits to similar disorders such as NPD, BD, PTSD and ADHD, to help more clearly differentiate the differences between these disorders. It described the somatic affects of chronic shame such as disgust, abandonment and rejection, as well as how to address this in therapy. It also presented an integrated model of healing BPD that includes a broad range of concepts, from Somatic Experiencing protocols, to supporting containment development and affect regulation. And finally, it addressed the complex aspect of counter-transference with a therapist’s own somatic awareness and how to work with that awareness to be more effective in working with a BPD client.
Footnotes
- [1]
- Clauer, J. (2012) Neurobiology and Developmental Aspects of Grounding., Bioenergetic Analysis, Clin. J. of IIBA, V21:38–40
- [2]
- Linehan M. (1993) Cognitive Behavior Therapy of Borderline Personality Disorder. New York: Guilford
- [3]
- Stepp, S. D. (2011) Children of Mothers with Borderline Personality Disorder: Identifying Parenting Behaviors as Potential Targets for Intervention. Personal Disord. Jan; 3(1): 76–91
- [4]
- Distal, M, et all (2009) Familial Resemblance of Borderline Personality Disorder Features: Genetic or Cultural Transmission? New York: Guilford
- [5]
- Kaess, M, et al (2014) Borderline Personality Disorder in Adolescence. Pediatrics, Official Journal of the American Academy of Pediatrics, V134(4)
- [6]
- Weill Cornell Medical Center (2007) Brain Abnormalities Underlying Key Element Of Borderline Personality Disorder Identified, Science Daily. www.sciencedaily.com/releases/2007/12/071221094757.htm
- [7]
- Ibid
- [8]
- Resneck-Sannes, H. (2002) Psychobiology of Affects: Implications for a Somatic Psychotherapy. Clin. J. of IIBA, V13:111–122
- [9]
- Gunderson, J. G., Hoffman, P. D. (2005) Understanding and Treating Borderline Personality Disorder. American Psychiatric Publishing, Inc. p. 7
- [10]
- Ibid 10
- [11]
- Ibid 6
- [12]
- Sarkis, S. (2011) Borderline Personality Disorder: Big Changes in the DSM-5. www.psychologytoday.com/blog/here-there-and-everywhere/201112/borderline-personality-disorder-big-changes-in-the-dsm-5
- [13]
- Ibid
- [14]
- Formica, M. J. (2008) Understanding Constancy in Relationship. Psychology Today. www.psychologytoday.com/blog/enlightened-living/200805/understanding-constancy-in-relationship.
- [15]
- Williams, K. (2016) I Hate You, Don’t Leave Me: Understanding the Borderline Personality. www.psychcentral.com/lib/i-hate-you-dont-leave-me-understanding-the-borderline-personality/.
- [16]
- Van Gelder, K. (2010) The Buddha and the Borderline: My Recovery from Borderline Personality Disorder through Dialectical Behavior Therapy. New Harbinger Publications
- [17]
- Borderline Personality Disorder Quotes. www.healthyplace.com/insight/quotes/borderline-personality-disorder-quotes/
- [18]
- Mason, P., Kreger, R. (2010) Stop Walking on Eggshells. New Harbinger Publications
- [19]
- Bentzen, M. (2015) Shapes of Experience: Neuroscience, Developmental Psychology, and Somatic Character Formation. The Handbook of Body Psychotherapy and Somatic Psychology, North Atlantic Books
- [20]
- Schroeter, V. (2009) Borderline Character Structure Revisited. Clin. J. of IIBA, V19:41
- [21]
- Borderline Narcissistic Personality Disorder Differences. https://www.clearviewwomenscenter.com/borderline-narcissistic-personality-disorder-differences.html
- [22]
- Marahi, A. J. (2008) Power and Control Struggles in Borderline Personality Disorder. www.borderlinepersonality.typepad.com/my_weblog/2008/07/power-and-contr.html
- [23]
- Lane, C. (2015) Borderline Personality Disorder. www.toddlertime.com/dx/borderline/bpd-ekleberry.htm
- [24]
- Gunderson, J. G., Hoffman, P. D. (2005) Understanding and Treating Borderline Personality Disorder. American Psychiatric Publishing, Inc. p. 43
- [25]
- Ford, J. D., Courtois, C. A. (2014) Complex PTSD, affect dysregulation, and borderline personality disorder. BioMed Central Ltd.
- [26]
- Urich, F. L. et al (2014) Neurobiology and Treatment of Traumatic Dissociation: Towards an Embodied Self. Springer Publishing Company, Pgs. 22–33
- [27]
- Ford, J. D., Courtois, C. A. (2014) Complex PTSD, affect dysregulation, and borderline personality disorder. BioMed Central Ltd.
- [28]
- Ibid
- [29]
- Ibid
- [30]
- Matthies, S. D., Philipsen, A. (2014) Common ground in Attention Deficit Hyperactivity Disorder (ADHD) and Borderline Personality Disorder (BPD): Review of Recent Findings. McGraw, A. P.
- [31]
- Wallen, D. J. (2007) Attachment in Psychotherapy. Gilford Press, pg. 49
- [32]
- Ibid 51
- [33]
- Ibid
- [34]
- Ibid
- [35]
- Ibid
- [36]
- Helfaer, P. M. (2007) Shame in the Light of Sex and Self-Respect. Clin. J. of IIBA, V17:57–79, pg. 66
- [37]
- Ibid 62, 67
- [38]
- Nathanson, D. L. (1994) Pride and Shame, Affect, Sex and the birth of Self. Norton & Co. Ltd.
- [39]
- Conger, J. (2001) The Body of Shame: Character and Play. Clin. J. of IIBA, V12:71
- [40]
- Nathanson, D. L. (1994) Pride and Shame, Affect, Sex and the birth of Self. Norton & Co. Ltd., pg. 49
- [41]
- Ibid 73–149
- [42]
- DeYoung, P. A. (2015) Understanding and Treating Chronic Shame: A Relational/Neurobiological Approach. Routledge, pg. xiii
- [43]
- Baum, S. (2007) Living On Purpose: Reality, Unreality and the Life of the Body. Clin. J. of IIBA, V17, Pg. 157
- [44]
- Maley, M. (2002) Bioenergetic Fundamentals, A Self-Exploration Manual. Body Smart Publications, pg. 22–23
- [45]
- Schroeter, V. (2009) Borderline Character Structure Revisited. Clin. J. of IIBA, V19:46
- [46]
- Ibid 48
- [47]
- Clauer, J. (2012) Neurobiology and Developmental Aspects of Grounding. Bioenergetic Analysis. Clin. J. of IIBA, V21:100–103
- [48]
- Schroeter, V. (2009) Borderline Character Structure Revisited. Clin. J. of IIBA, V19:46
- [49]
- Berceli, D. (2005) Trauma Releasing Exercises (TRE): A revolutionary new method for stress/trauma recovery. Book Surge Publishing. www.traumaprevention.com
- [50]
- Pederson, L. (2015) Dialectical Behavior Therapy: A Contemporary Guide for Practitioners. Wiley-Blackwell
- [51]
- Aung, S. K. H., Heather, F., & Hobbs, R. F. (2013) Traditional Chinese Medicine as a Basis for Treating Psychiatric Disorders: A Review of Theory with Illustrative Cases. Medical Acupuncture, Mary Ann Liebert, Inc.
- [52]
- Ortner, N. (2014) The Tapping Solution. Hay House Inc. 8th ed.
- [53]
- Andrade, J., & Feinstein, D. (2004) Energy Psychology: Theory, Indications, Evidence. In D. Feinstein, Energy psychology interactive Innersource, Appendix 199–214
- [54]
- Feinstein, D., & Eden, D. (2008) Six pillars of energy medicine: Clinical strengths of a complementary paradigm. Alternative Therapies, V14(1): 44–54
- [55]
- Levitt, J. T., Cloitre, M. (2005) A clinician’s guide to STAIR/MPE: Treatment for PTSD related to childhood abuse. Cognitive and Behavioral Practice V12(1):40–52
- [56]
- Ford, J. D., Russo E. (2006) Trauma-focused, present-centered, emotional self-regulation approach to integrated treatment for posttraumatic stress and addiction: trauma adaptive recovery group education and therapy (TARGET). American Journal of Psychotherapy V60(4):335–55
- [57]
- Shapiro, B. (2008) Your Core Energy is Within Your Grasp. Clin. J. of IIBA, V18:65-91
- [58]
- Shapiro, B. (2006) Bioenergetic Boundary-Building. Clin. J. of IIBA, V16: 155–178
- [59]
- Levine, P. A. (1997) Waking the Tiger. North Atlantic Books
- [60]
- Ibid. 199
- [61]
- Yalom, V., Yalom, M. (2010) Peter Levine on Somatic Experiencing. www.psychotherapy.net/interview/interview-peter-levine
- [62]
- Carlton, J. A. (2009) Somatic Treatment of Attachment Issues: Applying Neuroscientific and Experimental Research to the Clinical Situation. CA-SPR (Canadian Society for Psychotherapy Research) Montreal
- [63]
- Levine, P. A. (1997) Waking the Tiger. North Atlantic Books, pg. 199
- [64]
- Helfaer, P. M. (2007) Shame in the Light of Sex and Self-Respect. Clin. J. of IIBA, V17:74
- [65]
- Ibid
- [66]
- Cryns, Ingrid (2012) EMF & Radiation FAQ’s. www.somaearth.com/emf-radiation-faqs/
- [67]
- Lane, C. (2015) Borderline Personality Disorder. www.toddlertime.com/dx/borderline/bpd-ekleberry.htm
- [68]
- Ibid
- [69]
- Ibid
- [70]
- Ibid
- [71]
- Baum, S. (2007) Living On Purpose: Reality, Unreality and the Life of the Body. Clin. J. of IIBA, V17:178–182
- [72]
- Rogers, M., McKay, D. J. (2003) When Anger Hurts: Quieting the Storm Within. New Harbinger Publications, Pg. 27
- [73]
- Cutler, N. (2011) Anger Inflames Liver Disease. www.liversupport.com/anger-inflames-liver-disease/
- [74]
- Bentzen, M. (2015) Shapes of Experience: Neuroscience, Developmental Psychology, and Somatic Character Formation. The Handbook of Body Psychotherapy and Somatic Psychology, North Atlantic Books
- [75]
- Ford, J. D., Courtois, C. A. (2014) Complex PTSD, affect dysregulation, and borderline personality disorder. BioMed Central Ltd.
References
Andrade, J., & Feinstein, D. (2004) Energy Psychology: Theory, Indications, Evidence. In D. Feinstein, Energy psychology interactive, Innersource, Appendix 199–214
Aung, S. K. H., Heather, F., & Hobbs, R. F. (2013) Traditional Chinese Medicine as a Basis for Treating Psychiatric Disorders: A Review of Theory with Illustrative Cases. Medical Acupuncture, Mary Ann Liebert, Inc.
Baum, S. (2007) Living On Purpose: Reality, Unreality and the Life of the Body. Clin. J. of IIBA, V17
Bentzen, M. (2015) Shapes of Experience: Neuroscience, Developmental Psychology, and Somatic Character Formation. The Handbook of Body Psychotherapy and Somatic Psychology, North Atlantic Books
Berceli, D. (2005) Trauma Releasing Exercises (TRE): A revolutionary new method for stress/trauma recovery. Book Surge Publishing. www.traumaprevention.com
Carlton, J. A. (2009) Somatic Treatment of Attachment Issues: Applying Neuroscientific and Experimental Research to the Clinical Situation. CA-SPR (Canadian Society for Psychotherapy Research) Montreal www.jacquelineacarletonphd.com/text/pdfs/somatictreatmentofattachmentissues.pdf
Chapman, A. L. (2006) Dialectical Behavior Therapy, Current Indications and Unique Elements. Psychiatry, Edgemont
Clauer, J. (2012) Neurobiology and Developmental Aspects of Grounding. Bioenergetic Analysis, Clin. J. of IIBA, V21:38–40
Conger, J. (2001) The Body of Shame: Character and Play. Clin. J. of IIBA, V12: 71–85
DeYoung, P. A. (2015) Understanding and Treating Chronic Shame: A Relational/Neurobiological Approach. Routledge
Distal, M., Rebollo-Mesa, I., et al (2009) Familial Resemblance of Borderline Personality Disorder Features: Genetic or Cultural Transmission? PLoS ONE V4(4): e5334. DOI: https://doi.org/10.1371/journal.pone.0005334
Feinstein, D., & Eden, D. (2008) Six pillars of energy medicine: Clinical strengths of a complementary paradigm. Alternative Therapies, V14(1): 44–54. www.innersource.net/em/107-resources/publishedarticles/283-sixpillarsofem-dp1.html
Ford, J. D., Courtois, C. A. (2014) Complex PTSD, affect dysregulation, and borderline personality disorder. BioMed Central Ltd. www.ncbi.nlm.nih.gov/pmc/articles/PMC4579513/
Ford, J. D., Russo E. (2006) Trauma-focused, present-centered, emotional self-regulation approach to integrated treatment for posttraumatic stress and addiction: trauma adaptive recovery group education and therapy (TARGET). American Journal of Psychotherapy V60 (4): 335–55
Gunderson, J. G., Hoffman, P. D. (2005) Understanding and Treating Borderline Personality Disorder. American Psychiatric Publishing, Inc. ISBN 978-1-58562-135-4
Helfaer, P. M. (2007) Shame in the Light of Sex and Self-Respect. Clin. J. of IIBA, V17: 57–79
Kaess, M., Brunner, R., Chanen, A. (2014) Borderline Personality Disorder in Adolescence. Pediatrics, Official Journal of the American Academy of Pediatrics, V134 (4) www.pediatrics.aappublications.org/content/134/4/782
Linehan M. (1993) Cognitive Behavior Therapy of Borderline Personality Disorder. Guilford Press
Levine, P. A. (1997) Waking the Tiger. North Atlantic Books. www.traumahealing.org
Levitt, J. T., Cloitre, M. (2005) A clinician’s guide to STAIR/MPE: Treatment for PTSD related to childhood abuse. Cognitive and Behavioral Practice V12 (1): 40–52 ·DOI: 10.1016/S1077-7229 (05) 80038-0
Maley, M. (2002) Bioenergetic Fundamentals, A Self-Exploration Manual. Body Smart Publications
Mason, P., Kreger, R. (2010) Stop Walking on Eggshells. New Harbinger Publications
Matthies, S. D., Philipsen, A. (2014) Common ground in Attention Deficit Hyperactivity Disorder (ADHD) and Borderline Personality Disorder (BPD): Review of Recent Findings. McGraw, A. P. DOI: https://doi.org/10.1186/2051-6673-1-3
Nathanson, D. L. (1994) Pride and Shame, Affect, Sex and the birth of Self. Norton & Co. Ltd.
Ortner, N. (2014) The Tapping Solution. Hay House Inc. 8th Ed.
Pederson, L. (2015) Dialectical Behavior Therapy: A Contemporary Guide for Practitioners. Wiley-Blackwell
Resneck-Sannes, H. (2002) Psychobiology of Affects: Implications for a Somatic Psychotherapy. Clin. J. of IIBA, V13: 111–122
Rogers, M., McKay, D. J. (2003) When Anger Hurts: Quieting the Storm Within. New Harbinger Publications
Schroeter, V. (2009) Borderline Character Structure Revisited. Clin. J. of IIBA, V19: 31–51
Shapiro, B. (2006) Bioenergetic Boundary-Building. Clin. J. of IIBA, V16: 155–178
Shapiro, B. (2008) Your Core Energy is Within Your Grasp. Clin. J. of IIBA, V18: 65–91
Stepp, S. D. (2011) Children of Mothers with Borderline Personality Disorder: Identifying Parenting Behaviors as Potential Targets for Intervention. Personal Discord V3 (1): 76–91 DOI: https://doi.org/10.1037/a0023081
Urich, F. L. et al (2014) Neurobiology and Treatment of Traumatic Dissociation: Towards an Embodied Self. Springer Publishing Company
Van Gelder, K. (2010) The Buddha and the Borderline: My Recovery from Borderline Personality Disorder through Dialectical Behavior Therapy. New Harbinger Publications
Wallen, D. J. (2007) Attachment in Psychotherapy. Gilford Press
Warren C, et al. (2012) Too close for comfort, or too far to care? Finding humor in distant tragedies and close mishaps. Psychological Science Journal, Sage Publications. ISSN 1467-9280 www.ncbi.nlm.nih.gov/pubmed/22941877
Wolke, D, Schreier A, et al. (2012) Bullied by peers in childhood and borderline personality symptoms at 11 years of age: A prospective study. The Journal of Child Psychology and Psychiatry. V53(8):846–855 https://www.ncbi.nlm.nih.gov/pubmed/22380520
Website Articles
Borderline Personality Disorder. www.outofthefog.website/personality-disorders-1/2015/12/6/borderline-personality-disorder-bpd
Borderline Narcissistic Personality Disorder Differences. www.clearviewwomenscenter.com/borderline-narcissistic-personality-disorder-differences.html
Borderline Personality Disorder Quotes. www.healthyplace.com/insight/quotes/borderline-personality-disorder-quotes/
Cryns, Ingrid (2012) EMF & Radiation FAQ’s. www.somaearth.com/emf-radiation-faqs/
Cutler, N. (2011) Anger Inflames Liver Disease. www.liversupport.com/anger-inflames-liver-disease/
Formica, M. J. (2008) Understanding Constancy in Relationship. www.psychologytoday.com/blog/enlightened-living/200805/understanding-constancy-in-relationship.
p Lane, C. (2015) Borderline Personality Disorder. Psyweb.com. www.toddlertime.com/dx/borderline/bpd-ekleberry.htm
Marahi, A. J. (2008) Power and Control Struggles in Borderline Personality Disorder. www.borderlinepersonality.typepad.com/my_weblog/2008/07/power-and-contr.html
Neale, S. (2016) Stop Walking on Eggshells: Taking Your Life Back When Someone You Care About Has Borderline Personality Disorder. www.psychcentral.com/lib/stop-walking-on-eggshells-taking-your-life-back-when-someone-you-care-about-has-borderline-personality-disorder/
Sarkis, S. (2011) Borderline Personality Disorder: Big Changes in the DSM-5. www.psychologytoday.com/blog/here-there-and-everywhere/201112/borderline-personality-disorder-big-changes-in-the-dsm-5
Weill Cornell Medical Center (2007) Brain Abnormalities Underlying Key Element Of Borderline Personality Disorder Identified. www.sciencedaily.com/releases/2007/12/071221094757.htm
Williams, K. (2016) I Hate You, Don’t Leave Me: Understanding the Borderline Personality. www.psychcentral.com/lib/i-hate-you-dont-leave-me-understanding-the-borderline-personality/
Yalom, V., Yalom, M. (2010) Peter Levine on Somatic Experiencing. www.psychotherapy.net/interview/interview-peter-levine
About the Author
Ingrid Cryns, BES, B Arch, CBT, has a private practice in Toronto, Newmarket and Zephyr, Ontario. She has been a Certified Bioenergetic Therapist since 2004. Ingrid has written poetry, published articles on psychotherapy, regularly posts blogs and has taught a wide variety of webinars, seminars and workshops for over 15 years.
Ingrid Cryns, BES, B Arch, CBT
866-888-7662
Email: ingrid@buildingsoul.ca