Polyvagal Theory
Introduction for Somatic Psychotherapy
Vincentia Schroeter
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2016 (26), 9–40
https://doi.org/10.30820/0743-4804-2016-26-9 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstracts
English
This paper introduces polyvagal theory (1995) as defined by its originator, Stephen Porges, for the benefit of somatic, body-oriented, clinical psychotherapists. While there has been a recent explosion of interest in integrating this psychophysiological theory within various fields, some of the references to and explanation of the material can be difficult to grasp. The goal of this paper is to provide a clear explication of this theory. The main tenets of polyvagal theory will be presented including neuroception, the old and new view of the autonomic nervous system (ANS), normal and stress functions of the ANS, and trauma and attachment from a polyvagal point of view. Case material will illustrate somatic relational techniques from an ANS lens. The use of anatomical portals to contact or promote shifts will be provided.
Key words: polyvagal, neuroception, autonomic nervous system, sympathetic, social engagement system, vagal brake, portals
German
Dieser Beitrag gibt für somatische, körper-orientierte und klinische Psychotherapeut/innen eine Einführung in die Polyvagal-Theorie, wie sie von ihrem Begründer Stephen Porges entwickelt wurde. Während in jüngster Zeit ein explodierendes Interesse an der Integration dieser psychophysiologischen Theorie auf verschiedenen Gebieten zu verzeichnen war, sind einige Hinweise auf und Erklärungen zu dem betreffenden Material schwer zu verstehen. Ziel dieses Beitrags ist es, eine klare Darstellung der Theorie zu liefern. Es werden die hauptsächlichen Konzeptualisierungen der Polyvagal-Theorie vorgetragen, einschließlich der Neurozeption, der alten und einer neuen Sichtweise des Autonomen Nervensystems (ANS), normale und Stress-bedingte Funktionsweisen des ANS, Trauma und Bindung aus einer polyvagalen Perspektive. Fallbeispiele illustrieren beziehungsorientierte, körperpsychotherapeutische Techniken aus einem ANS-bezogenen Blickwinkel. Die Nutzung anatomischer Portale, um Veränderung wahrzunehmen oder zu initiieren, wird erläutert.
French
Cet article présente la théorie polyvagale telle que son concepteur, Stephen Porges (1995), l’a définie, constituant un apport majeur pour les psychothérapeutes, qu’ils soient d’orientation psychosomatique ou psychocorporelle. Il existe aujourd’hui un extraordinaire intérêt à intégrer cette théorie psychophysiologique dans ces divers champs, mais quelques unes de ses références ou de ses explications peuvent rester difficiles à saisir. L’objectif de cet article est d’en proposer une vision claire. Les grands principes de la théorie polyvagale y seront présentés, incluant la neuroception, l’ancienne et la nouvelle appréhension du système nerveux autonome (SNA), les fonctions du SNA normales et relatives au stress, une vision du trauma et de l’attachement du point de vue polyvagal. Des cas cliniques illustreront des techniques somatiques-relationnelles passées par le filtre du SNA. L’utilisation de portails anatomiques sera proposée afin de promouvoir le changement.
Spanish
Este ensayo introduce la teoría polivagal (1995) tal y como la define su creador, Stephen Porges, para el beneficio de los psicoterapeutas clínicos de orientación somática del cuerpo. Aunque ha habido una reciente explosión de interés en la integración de esta teoría psicofisiológica en diversos ámbitos, algunas de las referencias sobre la explicación del material pueden ser difíciles de entender. El objetivo de este ensayo es el de proporcionar una aclaración acerca de esta teoría. Se presentarán los postulados principales de la teoría polivagal, incluyendo la neurocepción, las consideraciones antiguas y nuevas sobre el sistema nervioso autónomo (SNA), las funciones normales y estresadas del SNA, y el tema del trauma y el apego desde un punto de vista polivagal. El material de los casos prácticos ilustrará las técnicas relacionales somáticas a través de las lentes del SNA. Se proporcionará el uso de portales anatómicos para contactar o promover cambios.
Portuguese
Este artigo apresenta a Teoria Polivagal (1995), tal como é definida por seu fundador, Stephen Porges, no intuito de auxiliar psicoterapeutas que seguem orientações clínicas somáticas e corporais. Embora haja uma recente explosão de interesse em integrar esta teoria psicofisiológica com diversos campos, algumas referências e explicações desse material podem ser de difícil entendimento. O objetivo deste artigo é fornecer uma explicação clara desta teoria. Serão apresentados, aqui, os princípios fundamentais da Teoria Polivagal, incluindo neurocepção, a antiga e a nova visão do Sistema Nervoso Autônomo (SNA), funções normal e de stress do SNA e trauma e apego a partir do ponto de vista polivagal. Material de estudos de caso ilustram técnicas somático-relacionais através da lente do SNA, assim como se demonstra o uso de portais anatômicos relativos ao contato ou à promoção de mudanças.
I. Introduction
Interest in polyvagal theory has been spreading as it lends a valuable new view of human behavior from a neurological point of view. Within psychology, polyvagal theory has broad clinical applications and has influenced the understanding and treatment of many issues including trauma, personality disorders, and childhood challenges, such as autism. While many psychotherapists are integrating Polyvagal Theory into their clinical understanding and practice (including articles in this journal: see Heinrich-Clauer (2016), Shahri (2014, 2017), Clauer (2016), also Clauer workshop, IIBA conference (2011), the theoretical information can appear complex, particularly due to the dense writing of the book introducing polyvagal theory by it’s originator, Stephen Porges. The book, The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, Self-Regulation is available in English, German (published in 2010) and is currently being translated into Italian.
Since its publication (2011), Porges has become a sought after and clearer communicator as interest in his research has exploded into and benefited many fields, such as neurology, medicine, biology, education, psychology, communication, and mindfulness. Others (notably John Chitty) have interpreted his work for psychology in an easier to grasp fashion. Some of Chitty’s visual material (used by permission) will be included in this paper. This paper proposes to add to the clarification of terms and concepts for the benefit of psychotherapists who wish to become more familiar with polyvagal theory and to apply it to the clinical setting.
A. Bioenergetics and the Historical Centrality of the Body
Bioenergetics as developed by Alexander Lowen (1957) has always placed the body, along with its arousal and regulation at the center of therapeutic action. Lowen’s predecessor, Wilhelm Reich (1930), observed that the body responds automatically and defensively to states of emotional arousal, painful or pleasurable, and that the body and its patterns of armoring should therefore be central in psychoanalytic inquiry and intervention. The unity of psyche and soma with the soma (body) as the main target of intervention was rejected by Freud and most of his followers. Reich observed and defined various body-types as responses in characteristic patterns of tension (character types), which arise from developmental wounding. While Reich’s theoretical ideas were lauded and studied in psychoanalytic circles for many years (Character Analysis, 1933), the bridge from theory to working somatically as the central technique to healing was never widely accepted. So Reich created his own school (The School of Social Research) to teach his method, and Bioenergetics was the next generation of his work.
Other somatic psychotherapies focusing on the body sprang up over the years, such as Feldenkrais, Hellerwork, and Radix, but none with the same strong ties to psychoanalytic understanding as Bioenergetics. The developmentally adaptive organism as manifest in the physical body, (even with application of modern shifts in psychodynamic theory), has always been at the main center of therapeutic focus in Bioenergetics. The emphasis is on mobilizing the organism away from defensive and toward healthy emotional and affective processes as they are seen in the body.
While the emphasis has been to mobilize the organism away from defensive, destructive processes and toward emotionally healthy processes, it is polyvagal theory that sheds a light on the inner workings of the nervous system in a way that helps us understand more deeply the mechanisms of defense and healthy emotional communication on a body level. Following a short introduction to Porges, parts of an interview will be presented. In the interview Porges supports the somatically oriented psychotherapist as the only clinician who does not just work “top-down” (from head to body only) and who understands the bi-directional communication of body and brain that he (Porges) has now scientifically backed up by his theory.
B. Introduction to Stephen Porges’ Theory
1. Background
Stephen W. Porges is a neuroscientist interested in the neurobiology of human behavior. He is a university scientist at the Kinsey Institute at Indiana University and research professor of psychiatry in North Carolina, USA. Polyvagal Theory (hereafter referred to as PT) is a contribution to psychophysiology, which crosses many disciplines and is particularly relevant for somatic psychotherapy. Integrative studies linking the central nervous system (CNS) to autonomic function, such as PT (Porges, 1995, 2003) are new. Porges coined the term, “polyvagal” to emphasize three rather than the traditionally understood two branches of the ANS (Porges, 1995).
PT introduces a new perspective that:
- Relates autonomic function to behavior that sees the autonomic nervous system (ANS) as a “system.”
- Identifies neural circuits involved in regulating autonomic states.
- Interprets autonomic reactivity as adaptive from a phylogenetic perspective.
Porges created a groundbreaking contribution to our understanding of the human organism in terms of how our nervous system functions and how it regulates our visceral system. As part of the explosion of research in neuroscience, he has provided new links and confirmed heretofore mystical connections between the brain, the organs and affective parts of the body. For instance, they really do communicate back and forth! The bi-directional communication of organs to brain, as well as brain to body is revolutionary. PT also adds to our understanding of the reactivity of humans, particularly under stress. Since publishing his seminal book (2011), Porges has continued his mission to do scientific research and to communicate his new understanding of the ANS (Automatic Nervous System) as it applies to many fields. His own website www.stephenporges.com has many articles, interviews and videos.
Although his book can be dense and repetitive, it contains valuable physiological detail that will not be included in this paper. Next, are some notes from an interview with Porges where he supports the somatic psychotherapy world as respecting the bi-directional travels of brain and body communication.
2. The Nervous System and Visceral Feelings
Here are some notes from Serge Prengel’s interview of Porges (www.somaticperspectives.com):
Serge Prengel: How does our nervous system interplay with our visceral feelings?
Stephen Porges: Although the important role that the nervous system plays in regulating our visceral state and thus our feelings is a relevant question for people interested in body psychotherapy, it is not even acknowledged in many of the models, theories, and therapies emphasized in clinical psychology and psychiatry. Clinical psychology and psychiatry primarily use top-down models that focus on emotions and affective processes as being central phenomena and minimize the role of the body in the experience. For example, consistent with these models, even anxiety may be a “brain” process without a visceral manifestation. Fortunately, there are clinicians, including many body psychotherapists, who have an appreciation of the importance of the bidirectional communication between the brain and the body. For example, sensory information travels from the body to the brain and influences how we respond to the world. And brain processes can influence our viscera via the cognitive and affective processes related to our perspective of the world and our reactions to various features of the environment. This bidirectional and interactive notion of how our nervous system regulates our viscera in a complex social environment, although intuitive, is neglected or minimized by much of clinical medicine including psychiatry.
So Porges is acknowledging body psychotherapy at the forefront of the movement to incorporate this “bidirectional” communication between body and brain. In his book he writes about the efferent (from brain down) and afferent (from the organs up to the head) communication that exists. The neglect he speaks of is changing in many circles, as we digest and incorporate this valuable knowledge from polyvagal theory. The main concepts of this theory are covered next.
3. Triune Brain
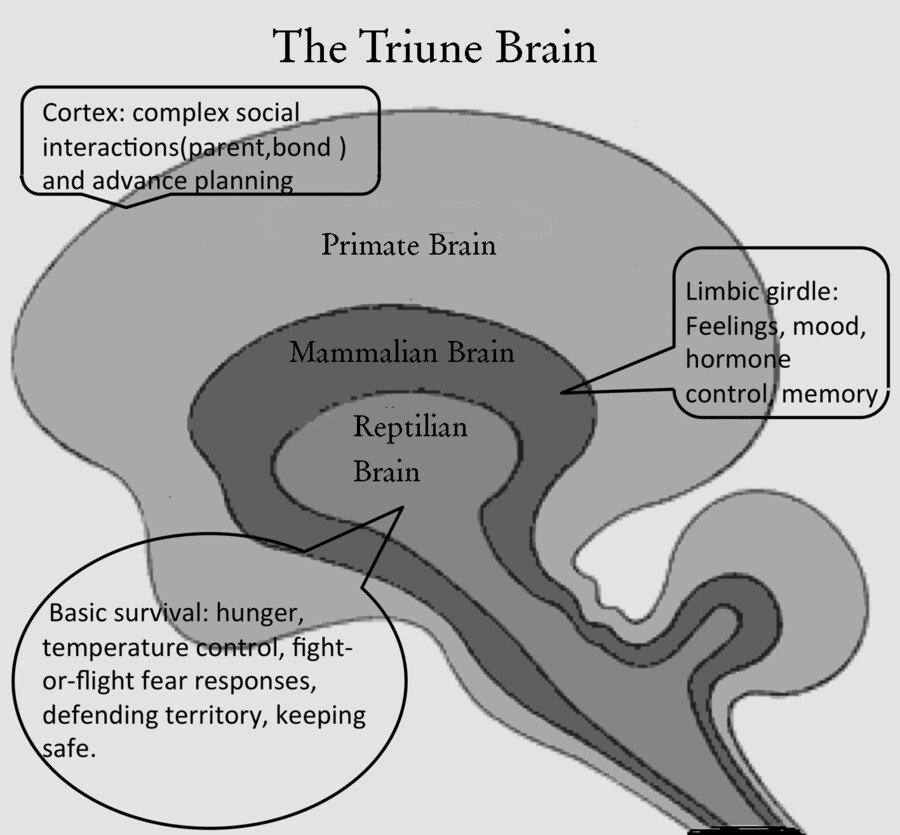
Figure 1. The Triune Brain
The triune brain is made up of the brainstem, which houses the most primitive reptilian brain; the limbic, shared with other mammals; and the neo-cortex, that primates have and is most developed in humans.
II. Main Concepts: Polyvagal Theory
A. Neuroception
1. Introduction to Neuroception
This term was coined by Porges to define an automatic process. Neuroception is an unconscious detection of safety or danger. For example, when we are in nature, we may see what looks like a snake on the road. We immediately freeze in an alert state. We do not go closer until we assess that it is just a stick and not a dangerous snake. The automaticity of the response is evolutionarily adaptive for when quick action is needed to survive danger. The “survival of the fittest” was a term coined by Spencer (1864). In groups this survival depended on both trust and bonding with others and also this neuroception of danger. If the tiger is heard or an enemy tribe spotted, instant reaction could be the difference between life and death. Our ancestors who wanted to think too long before acting in crisis situations like life threat, probably died. Those that lived on, these survivors, carried neuroception prowess to succeeding generations.
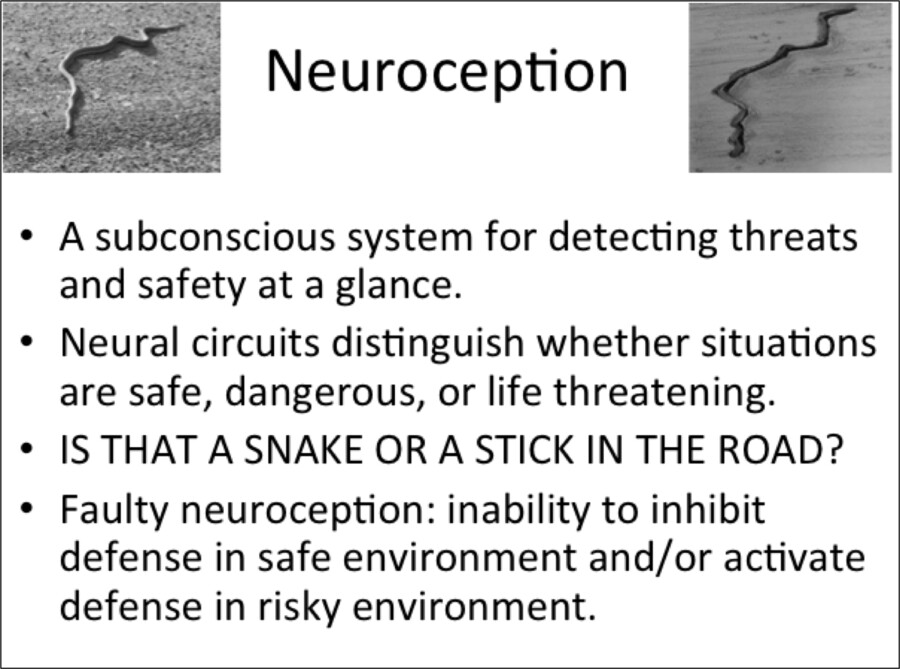
Figure 2. Neuroception Chart
2. Neuroception: Application to Psychotherapy
Neuroception is the unconscious assessment of safety versus danger that is part of the ANS. Understanding this instinct helps the client as well as the therapist feel compassion for choices that are made. Every choice can be seen through the useful lens of safety (perceived or real) versus danger (perceived or real). Faulty neuroception occurs when a person misperceives safety or danger. For instance, a person who lives in a generally safe neighborhood is afraid to walk outside their front door for fear of being accosted. This person sees danger where objectively there is none. On the other hand, feeling safe in a dangerous environment is also faulty neuroception. For example, walking down a dark alley in a carefree manner in a seedy neighborhood at night indicates a poor ability to neurocept or discern danger, where it exists.
3. Clinical Vignette Illustrating Neuroception
The following is provided to show an example of neuroception.
A female client who I have been seeing for years comes into her weekly session feeling happy, in a much better mood than last week, when she was depressed and not wanting to go for walks alone in her safe neighborhood. She did not want to venture out alone, even though she knew the exercise had potential to lift her depression. The reason was that she would see other happy couples and families on her walk. She was fearful the walk would provoke sadness at her recent relationship breakup. This caused her to contract, pull in toward herself and not take her walk outside. This pulling in is instinctive and feels protective due to the perceived danger of feeling the unwanted emotion of sadness. Her neuroception told her it was dangerous to go for a walk alone.
Perceived danger relates to a past trauma in her case. Dipping into sadness scares her because of her history. When her mother was dying she stopped eating, became catatonic, suffered severe depression, had a psychotic break and had to be hospitalized for an extended time. Although stable for many years, opening sadness triggers her fear of another psychotic break. Therefore, her avoiding the walk was a protection against a danger of decompensation.
B. ANS Old View versus New View
1. Introduction to New versus Old ANS View
Porges’ work changes what we learned about the autonomic nervous system from a dual antagonistic system (with two levels of response) to a hierarchical system with three levels of response to stimuli. The old view, the dual antagonistic system believed we go back and forth, like on a seesaw from hyperarousal (danger but not life threatening) to hypoarousal (life threat). The new view includes the important extra and evolutionarily newest branch, known as the SES (social engagement system). The three branches have different functions under normal conditions and under stress. The charts (used by permission) below were created by John Chitty (chapter 6, Dancing with Yin and Yang) and are clear illustrations of these three levels and their functions. According to Jackson’s theory of dissolution (see fig. 5), we use our phylogenetically newest system (SES) first UNDER STRESS, if it fails we use the next (SNS), if that fails we go to the most primitive system (PNS).
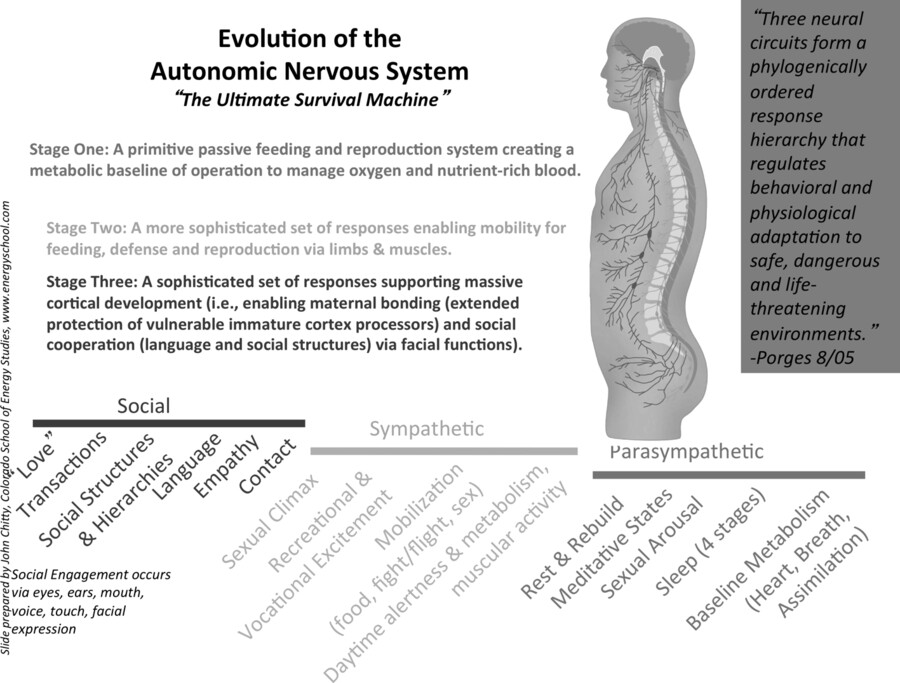
Figure 3. ANS 1
2. Normal Functions of ANS
The chart (see fig. 3: ANS 1) shows the normal functions of the three parts of the ANS. The ANS evolved in three stages over time. Stage one, is the oldest phylogenetically and most primitive. We share this system, the parasympathetic, with reptiles. This has been referred to as, “the lizard brain.” Stage two, the sympathetic, occurs in animals further up the food chain, including mammals. This has been referred to as, “the mouse brain.” The most sophisticated system, stage three, is most highly developed in humans. This is the “new” area examined and highlighted by Porges in a way that has changed our thinking about the workings of the ANS.
3. Bonding Phylogeny
To illustrate all three levels, bonding with offspring will be used. Reptiles do not bond with their offspring. Once they are born babies instinctively move out into the world on their own. Animals, including birds and mammals, have a longer period of dependency on parents once they are born. Animals take care of their young by providing warmth, protection and feeding until the offspring can fend for themselves. The most recently formed is the social engagement system (aka “the communication system”). Although other mammals have some bonding and communication capacities like humans, this system is more developed in primates and is most developed in humans. Our young are dependent on caretaking longer than other animals, and therefore parents need sophisticated skills to keep them safe and babies need sophisticated skills to communicate their needs. We use our eyes, ears, voice, touch and facial expressions to maximize proximity for safety and bonding.
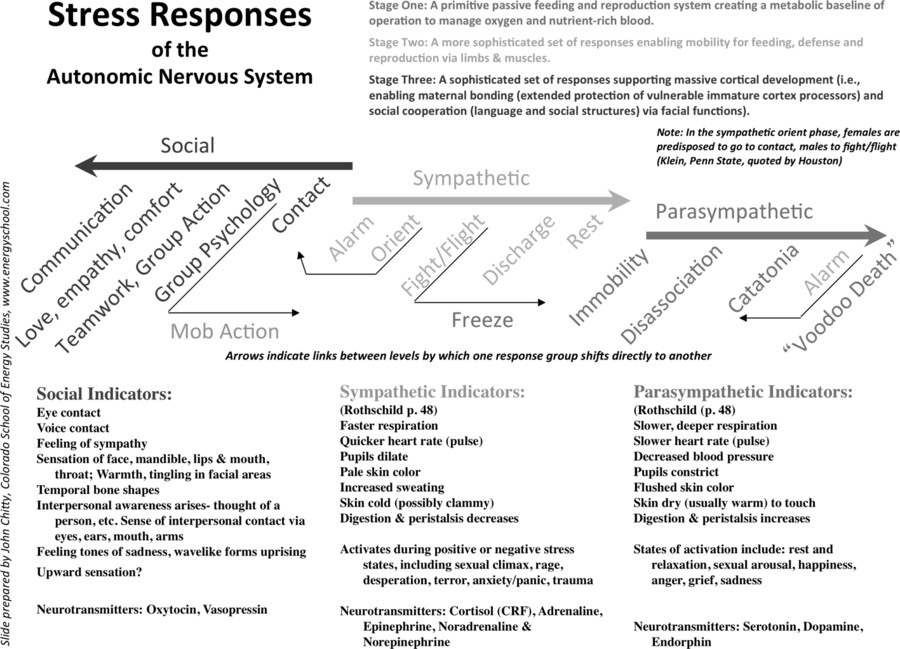
Figure 4. ANS 2
4. Stress Functions of the ANS
Figure 4: ANS 2 shows the stress response of the ANS. This is a crucial contribution to deepening our understanding of how the ANS operates in humans. The links show shifts from one system directly to another. For example, while the SES is usually a positive, calm yet engaged zone, where one feels safe and not under threat, notice that a strong identification with a group can cause a group psychology that solidifies into an “us against them” mentality that can make the group feel threatened, which can lead to a mob action. This automatically shifts the person into the SNS, ready to fight for the cause. An example might be a fundamental religious group that preaches tolerance, but feels so threatened by “non-believers” that they enter into a combative relationship with one group or another.
5. CAUTION: In Viewing Normal versus Stress ANS Figures
These charts (fig. 3: ANS 1 and fig. 4: ANS 2) show the normal and stress response of each level. It is important not to mix them up. In normal non-stress conditions each system has a job (see fig. 3: ANS 1 on normal functions). The normal PNS is for rest, relaxation, digestion, and immobilization without fear (as when we are in the arms of one we feel close to). The SES includes social warmth, a friendly animated face, voice prosody, listening, interacting, bonding, communication, and integrated thinking and feeling. The SNS is the charged and energized state we need when we are working, exercising, or learning in an alert and engaged manner.
6. Ladder of Dissolution
The next chart (see fig. 5: ANS 3) emphasizes the ladder, to show how we move automatically from one system to the next in descending order as stress increases. Jackson discovered this hierarchical order in 1850, before we had a term or common acceptance of the dynamics of the SES.
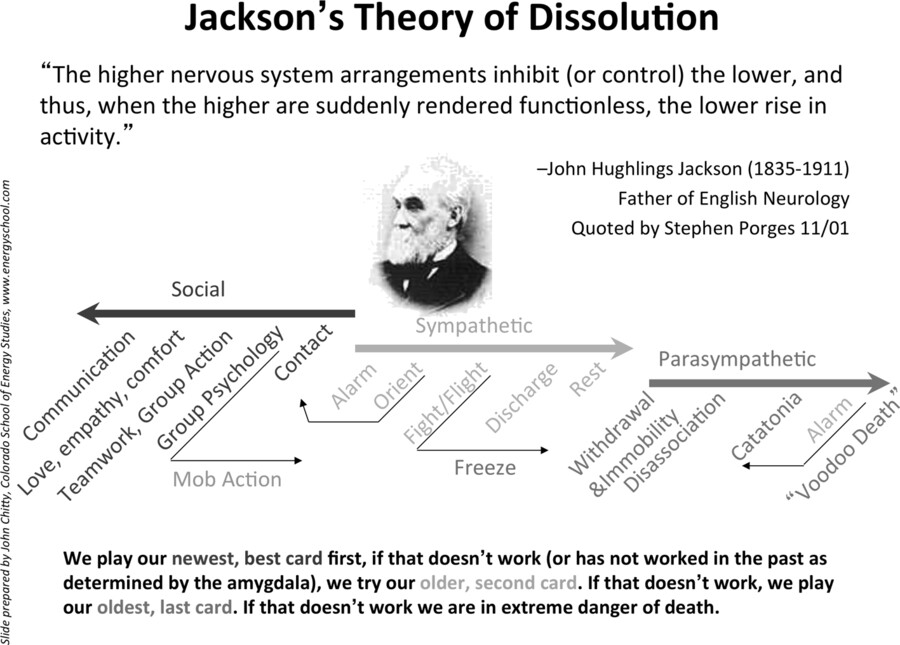
Figure 5. ANS 3
7. Subway Story (Dissolution Example)
For example, you smile at a person as you scoot in next to him to take a seat on the subway. These behaviors indicate you are in the SES. Your seatmate looks annoyed and moves away from you, pulling his belongings closer to him. Then he shoves you, telling you to get away from him. You immediately react by getting angry, and saying, “hey, stop that!” Or you could get up and get as far away from him as possible. Either way you are now in the SNS in fight or flight automatic response. But say you stayed in the seat, fuming. Next, your seatmate opens his coat, grabs a knife and traps you by grabbing your throat and threatening you with the knife. You freeze, as you have no other option. You are now in PNS, life threat response.
The subway confrontation story illustrates the attempt to use SES as the first “card.” When being friendly failed, the SNS (second card) was engaged. When the SNS fight response was met by a trapped feeling when the assailant pulled a weapon, the ANS dropped down immediately into the PNS as a freeze response to a life threat.
In fig. 5: ANS 3, Johnson is quoted as saying that the higher systems inhibit the lower. This means we try our best to function at a higher level. A history of trauma or abuse can weaken that capacity. This is because if we need to be constantly alert to danger and therefore spend much time in trauma states, we lose the neuroplasticity of the brain that gently calls upon the calmer, thinking brain to help us out. The safety blanket is thin and frayed, our need for love and healthy nurturing not fed. The brain prunes the branches so much that the SES is weak. However, people can increase their ability to build the SES. Once they do, it can act as an inhibitor to stop the impulsive actions of the SNS by way of the “vagal brake.”
8. The Vagal Brake
Although dissolution pressures are automatic, the SES can stop the SNS from acting automatically at times. The impulse to strike out in the throes of anger, when brought to awareness from an “online” thinking brain (in SES), allows the SES to put the brakes on the more impulsive SNS. To use the previous scenario, the seatmate on the subway example shoves you. You flare into instant distress, while considering fight or flight (the job of the SNS to protect you). In those few seconds you scan your environment and quickly assess the dynamics including your need to stay on the subway for three more stops, the unlikely chance you could get support or protection from others on the train, the trouble you might get in if you got angry at this time. Your vigilant eyes notice the dissociated look and very disheveled dress of your assailant. You size him up as being either in shock, drugged and/or mentally compromised at this time. The SES helps you decide not to fight, to pretend like you were not bothered, to apologize in order to hopefully calm him down, and to look for any open seats away from him. Slowly you move away when you can, willing to offer a smile if he looks at you.
This is an example of the SES ventral vagal complex (VVC) using tools to stop the automatic Fight/Flight response of the SNS. You have successfully utilized the vagal brake, which acted as restraint, or brake, limiting heart rate. As Porges writes, “Inhibitory (brake) effects of the VVC branch of vagus allow for a wide range of adaptive, prosocial behaviors” (ibid., p. 69). In essence the SES can act like an “intensity controller” (Samsel, n. d.) for arousal and doing. It affects mostly the heart keeping it humming at varying paces to match the amount of energy we need as those needs shift. A decrease in ventral vagal (up into SNS) frees up energy for activity in a precise and prompt way. So, for example, one can jump up off the couch when one has been sedentary to respond to a loud sound in the next room. Like a smooth new car, this makes for fluid shifting and balance between goal related activity and social activity (ibid.).
9. Old and New Model of ANS: Summary
- OLD MODEL: Two: Parasympathetic (PNS) or Sympathetic (SNS) reciprocate like on a seesaw, switched on/off, like a light.
- NEW MODEL: Three: hierarchical flow (try evolutionarily newest (SES) first). This phylogenetically formed, mammalian aspect is called the “Social Engagement System” (SES).
- SES helps mammals survive by engaging in protection, attraction, and group bonding.
- SAFETY or detection of safety (neuroception) is the ONLY road to SES. Once in SES, people engage comfortably, think clearly, can best learn and create.
| Aspect | Old View | New View |
| Importance | Under-appreciated | Supreme Importance |
| How many parts | Two (Sym-, Parasym-) | Three (Social, Sym-, Parasym-) |
| Action | Reciprocal (Sympathetic and Parasympathetic are seesaw, on/off) | Sequential based on phylogeny (evolutionarily newer vs. older) |
| ANS Categorization of Vagus Nerve | All Parasympathetic | Mixed (Ventral branch of Vagus is not Parasympathetic) |
| Therapy Goal | Parasympathetic relaxation | Re-establish newer branches |
| Babies | Feel no pain and have no memory | ANS is hyper-sensitive & records experiences, particularly betrayals |
| Popular characterization |
Parasympathetic “Rest & rebuild” Sympathetic “Fight or Flight” |
Differentiate “normal functions” from “stress functions” |
Figure 6 Old and New Views of ANS. (Recreated from Chitty, 2013 p. 119)
C. Trauma and Polyvagal Theory
1. Introduction
Polyvagal theory refines our understanding of trauma. It teaches us what happens internally in the nervous system and how our underlying visceral state colors our reactions. Porges’ theory is especially important for individuals and families who have experienced trauma because he normalizes the reactions people have to traumatic events. For example, dissociation is an adaptive (PNS) reaction when one is in a life-threatening situation. People can be relieved of feelings of shame to learn that their biology instinctively came up with the safest response to the danger. For example, people often wish they had gotten away when trapped by another, but they froze. They learn that their body instinctively assessed (using neuroception) that they could neither win that fight nor safely get away. When the body assesses a life threat it goes into a freeze state for the best likely outcome of survival.
2. Stimulus – Response and PT
Stimulus (S) information goes in and the body automatically responds (R) from the SNS, SES or PNS.
Figure 7. Stimulus-Response and Polyvagal Theory
When a person experiences chronic or severe trauma, there was often failure in the functioning of the SES, which is usually the first response to stimuli. This is likely because the traumatized person could not get the protection or help they needed to feel safe and easily recover. Disruption in their ability to access the SES for help changes brain pathways and creates a trauma response that could endure under new threats.
Samsel describes it this way:
The result of the trauma response is a spiral of autonomic and emotional dysregulation that produces progressive damage to the organism if not reversed. The main long-term effects are perpetrated through exaggerated swings between the sympathetic fight/flight system (SNS) and the dorsal vagal ‘freeze’ system (PNS). The latter may have been involved as the initial response to the traumatic events, or may have been recruited as a desperate brake on the spiraling sympathetic arousal system. These alternating aspects of this dysregulation are so hard on the body that they … (can cause chronic physical illnesses or conditions). (http://reichandlowentherapy.org/content/vegetative/dorsal_shift.html)
A trauma response seems to arise when very early efforts to regulate (return to SES) after a trauma are unsuccessful. This could be because the initial trauma was so great, like when the perpetrator was also an attachment figure or there was no one else to help you return to feeling safe. It could also be because social norms precluded outside comfort or the individual physical acts and emotional expressiveness required to “shake off” the early trauma response. In either case, the result is that those who suffer chronic trauma (with minimal experience of feeling protected or safe) often have a narrow window of tolerance for disturbing stimuli, producing fluctuations between hypo-and hyper-aroused states (Ogden, Minton, & Pain, 2006).
3. Clinical Example of Trauma Response
a. Presenting Problem
A male adult client came into his session hyperaroused, talking about work stress and his greed to make more and more money to build his successful business and fear of failing at that. This is a common theme. I mirror him and listen to his excitement and often get hyperaroused just listening to him. He is aware of being generally hyperaroused, working very long days. However he can also down regulate (from the SNS to the PNS) with regular yoga, meditation and a spiritual practice. But he tends to go from one extreme to the other (hyper or hypo), with difficulty in the middle (the SES). His wife complains that he does not share his emotions. He says he is a good listener but does not self-disclose to others. He admires people who can self-disclose and reports therapy is the only place he can be “genuine.”
He recently decided after his morning yoga, not to meditate, but to sit on the couch and spend time with his wife. She said it was nice that he listened but missed that he could not share his own feelings.
b. Intervention
To assess his level of emotional sharing and to practice (which can strengthen the communication level of the SES), I invited the client to tell me the first five feeling states he had experienced since the morning. To help out I started the sentence for him, “When I woke up I felt …” and he added, “tired.” I began again for him, “When I was driving I felt …” and he added, “I felt anxious.” He was able to do the rest himself: “in my first meeting I felt impatient, during a presentation I felt excited; dealing with a problem I felt confused.” I praise him for his efforts and he visibly relaxes. Feeling confident and safe he goes deeper discussing his trauma of being in a newborn incubator. He has scars around his belly and a hole in his back. He had four surgeries before age two to repair his lower gastrointestinal tract.
c. Insight
He pauses and makes the following link himself. “My greed (at work) is not related to money, but is related to fear of failure, that I won’t be enough.” He shared his insight that his fear as a child relates to his fear as an adult. So he could have compassion for his fear, I illustrated walking on a tightrope over a shark tank as someone asked me my feelings. I am in SNS fear, must move to survive, no time for the emotional world of SES. All I want is to get to the other side. For homework, he planned to do some centering and grounded breathing (to feel compassion for his trauma related fear) before sharing five feelings of the day with his wife.
d. Other Somatic Based Trauma Treatment
In terms of treatment, the work of Peter Levine (2010) and David Berceli (2005) specifically targets the trauma response, in large part through activation of movement including trembling. The trembling moves energy that needs completion so the effects of trauma can be resolved or reduced. The Reich and Lowen traditions have always included the activation of movement in the concept of body armor and organismic response to negating forces. (as in the Hilton diagram, 2008).
D.
Attachment and Polyvagal TheoryThe securely attached child moves flexibly between all three levels, to bond and seek safety using the SES, to explore through play (SNS/SES) and to rest safely in the arms of the parent (PNS). For a visual of circles of security and insecurity see fig. 2 on p. 113 (Schroeter, 2014 BA (24) p. 105–132). The insecure patterns have a smaller window of tolerance, or narrower range of time spent in the SES and are generally organized either lower in the PNS as hypoaroused), or high in the SNS as hyperaroused (ibid., p. 118, fig. 6). They can move quickly from high to low or vice versa, because the SES range is so narrow. The goal of clinical work is to expand the range of the SES. Clinical applications will be examined next.
III. Clinical Application and Tools
A. Threat Chart and PT
The Threat Chart was created by Tina Payne Bryson (co-author of The Whole Brain Child) to indicate where the brain goes under states of threat.
Although this copy is in black and white, the color version is useful for visual indication of arousal movement when stimulated by real or perceived states of threat. The top (Fear, Stress etc.) is the RED ZONE. When we get angry we “turn red” and if we get very angry we may erupt. So like a thermometer the hot zone is indicated in red. The top layer refers to the SNS. The middle zone is GREEN, indicating the bright, alert, emotionally balanced nature of the SES. This is the state that is wider and easier to move back to in securely attached people. The bottom is the BLUE zone. Blue is a color that can connote sadness or depression.
Remember, there are normal functions of the RED and BLUE zones. The words printed in this chart indicate what happens to the organism when we are in those zones AS A RESPONSE TO THREAT.
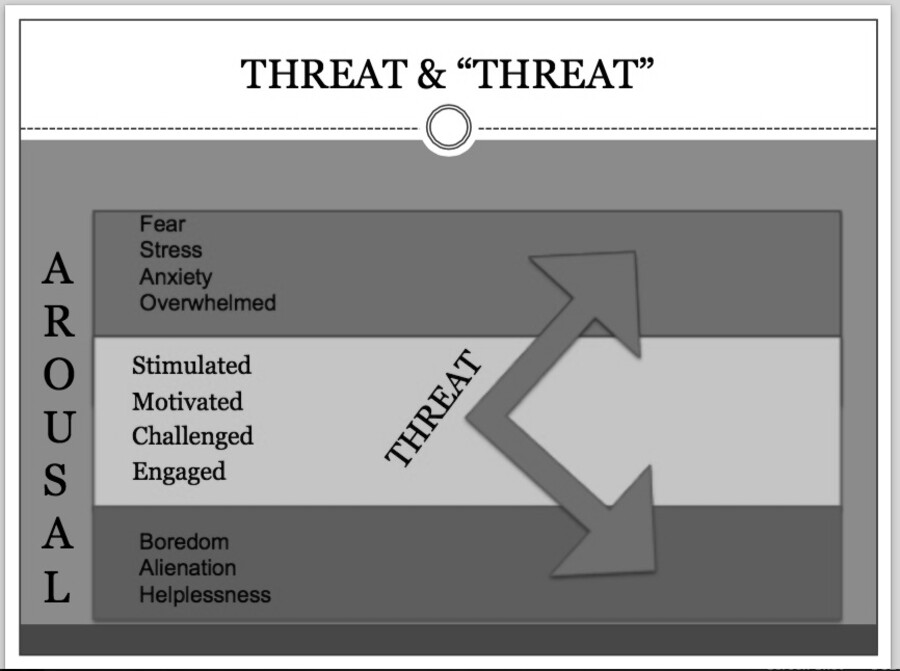
Figure 8. Threat and Arousal Chart
This chart (see fig. 8) is a simple and useful clinical tool. I have found that children as young as five years old, as well as adults can identify their arousal level. Even when they are in the RED or BLUE, where thinking functions poorly, clients can identify their arousal level. When presented with empathy and understanding, this chart becomes a tool to observe visceral states (or ANS states) and help bring clients back into the GREEN zone.
B. Arousal Zones with Normal and Stress Responses
Figure 9 combines arousal zones with cartoons of facial expressions typical of that zone. It is a tool to summarize the normal and stress functions of the ANS. Below is a clinical vignette illustrating Bioenergetic work to shift ANS states.
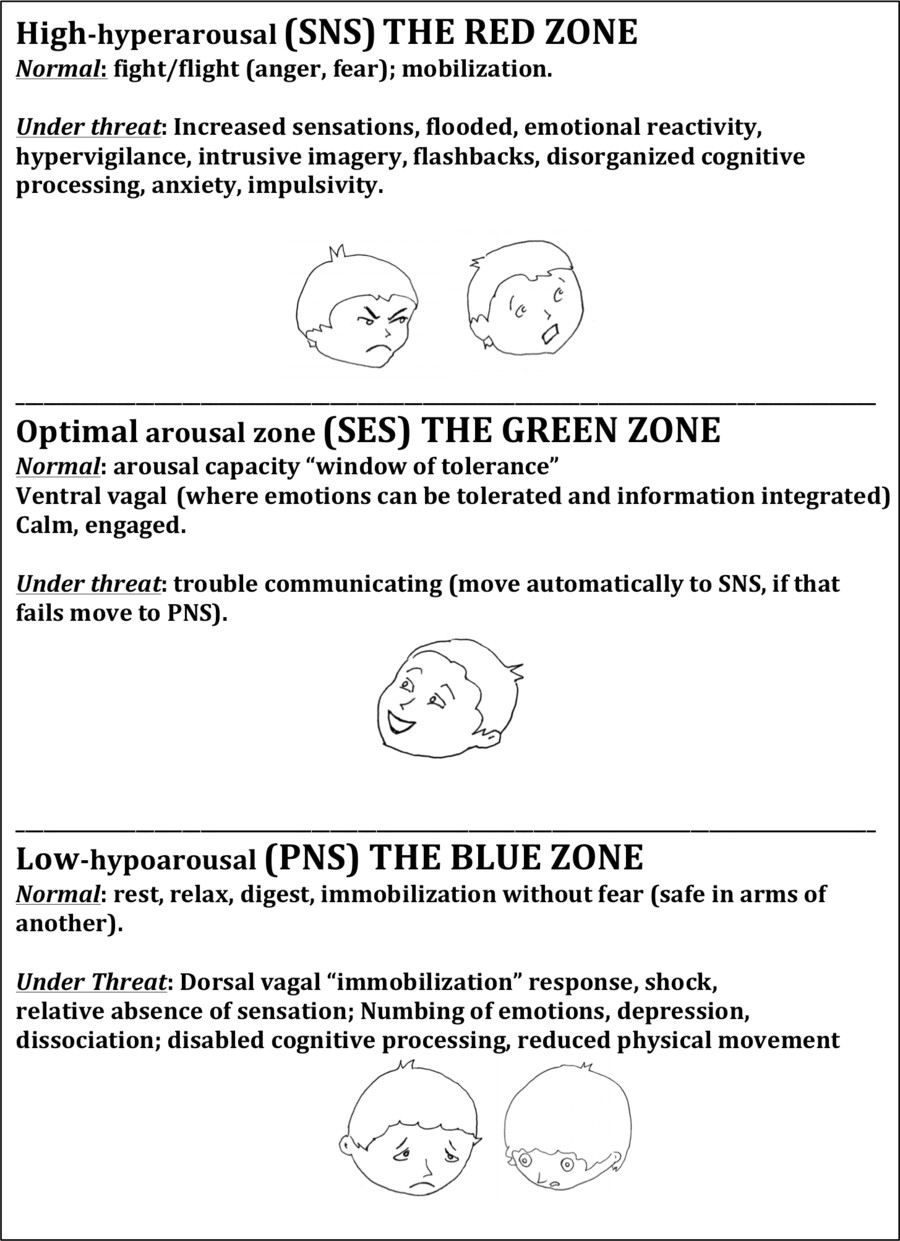
Figure 9. Chart adapted from Ogden, Minton and Pali (2006) and Corrigan, Fisher and Nutt (2010). Characters created and added by Vincentia Schroeter (2015)
1. Case Vignette: Bioenergetic Session, WOT and ANS State Shifts
The Window of Tolerance (WOT) is a concept coined by Dan Siegel (Siegel, 1999). A client stated her intention to solidify and expand a happy feeling she came in with by hitting with the heavy wooden bat on the mat in the office. First, she does some centering and grounding familiar to her that helps her feel gravity pull her to feeling more solid and feel her pelvis as an anchor to support her lower body. Once she has increased her charge, some pleasant shaking begins.
When she begins pounding the bat on the mat, she enjoys the movement until she hits a block in her diaphragm and throat. We do some breathing and voice work to help move through the block. As her voice is getting strong she is surprised by some anger. Next, sadness appears. She stays present (I am watching her eyes and monitoring the fluidity of her body movement to assess this level of presence). Anger comes through her eyes more as she stares at the pillow she is hitting. Discharging more anger brings the sadness to her face and her eyes droop. Opening the throat she continues with sound. Sounds change and sounds last longer. Soon sad “ohs” turn into sobbing as her diaphragm lets go. Next, she has an impulse to drop the bat, lean over and clutch a pillow. She follows these impulses and can feel her breath on the pillow, which she clutches with both hands.
Her energy has shifted. She feels contained, safer and in her words, “a new boundary” with cuddling, while leaning over the pillow. This allows deeper sobbing to emerge until she feels complete. She was surprised that opening up the charge brought anger and sadness. The mobility of engaging the SNS (using arm and back to hit) completes that movement and she drops more into affective sadness that she can own and feel good about. She has moved into the SES.
The client reports feeling more openness and reports, “I have never gone there before.” This indicates that the feeling of a wider SES is pleasant and new.
C. ANS Portals and Afferent Communication
1. Introduction
A concept arising from Porges’ work that has exciting clinical applications for somatic psychotherapists trained in anatomy is the use of “Portals” or points of entry to affect a change in the ANS branches. Chitty (2013) reports “ANS portals are anatomical components of the ANS that can be physically stimulated to support a particular layer. By stimulating a location in a special way, ANS change can be created” (p. 137). This means we can “reboot” the nervous system.
“Approximately 80% of the vagal fibers are afferent (originate from the body to affect the brain) and provide important information regarding visceral state … the vagal system becomes … a portal to neural systems in other parts of the brain … There is a strong neuroanatomical and neurophysiological justification to predict that stimulation of the vagal afferents would change activity of higher brain structures” (Porges, 2003).
This is very hopeful for bodyworkers and particularly somatic psychotherapists who are trained to follow the emotional aspects of changes in the nervous system. Stimulating any single afferent to the brainstem and limbic system will improve the whole nervous system. For example, Porges’ ongoing research providing acoustic stimulation to autistic children improves their communication and social interaction (Porges, 2008, 2011).
Bioenergetic therapists are not traditionally trained to focus on the workings of the nervous system. We are well trained in the workings of the muscular holding patterns and their mental and emotional results, both adaptive and maladaptive. We understand mobilization, immobilization and trauma in the body quite well. We have long professed that the body speaks to the brain and not just the brain to the body. We utilize varied hands on techniques to “move energy.” We see the effects of this movement of energy but perhaps can begin to describe it in a new way.
Understanding the previous principle that there are anatomical “portals” we can stimulate to affect this movement of energy in the ANS is exciting. With polyvagal theory, the nervous system comes more into view as an essential component in our work. We can use some of our techniques with a new understanding of how they affect the nervous system. Next, portals and techniques will be identified for each of the three parts of the ANS.
2. PNS Portals
The portal for the PNS, based on anatomy is the vagus nerve, accessible on both sides of the neck, and sacral plexus (L4–S4), which provides motor and sensory nerves for posterior thigh, lower leg, foot and part of the pelvis. Look at figure 3 to see where PNS nerves innervate (stimulate to action). Notice the many fibers sub (below) the diaphragm, indicating the lower part of the body, as well as some in the neck area. Therefore contact with the neck and lower back (lumbar-sacral area) will stimulate the PNS and help restore it’s functions. For example, when you stretch your neck gently or get a neck massage it is often very relaxing. Relaxation is the royalty of the PNS. Contact with the lower back (lower lumbar and sacral regions) can innervate the lower body, including the pelvic area (relaxes the perineum), increases peristalsis (digestion) and restores normal bladder and rectal function. Again, we have to be relaxed for digestion and elimination to function optimally.
3. PNS Portal Technique
This reminds me of two touch techniques that Mae Nascimento (2014) introduced in her article (BA, 24,11–31). The point of her paper was to utilize techniques that “create a more introspective nature, helping the connection with the energy flow” (ibid., p. 29). Because they address the PNS, I will quote from her paper here:
A. LUMBAR TOUCH
The therapist must be at the client’s side so that he can observe his reactions and ask him from time to time what is going on.
With the client in a grounding position (standing with knees slightly bent), stand behind the client and touch the lumbar zone of the vertebral column between the fourth and fifth vertebrae with the index and middle fingers and the palm of your hand facing down toward the floor. The client is asked to breathe so that he can keep the focus upon what happens within himself.
‘It is a physical touch … that reaches the energetic flow through the nervous system and not through the bone structure or muscular layers … this touch activates the energy through the autonomous nervous system and by resonance over the sensory and emotional fields. It also activates the perineum and the Hara*, facilitating an internal grounding and a deep plunging within oneself’ (Basso & Pulstilnik, 2001, p. 49–50).
(*Centro Hara – by which the mother’s blood fed us through the umbilical cord and where we get our blood nutrition through our digestive process (Basso & Pulstilnik, 2001, p. 50).
B. CERVICAL TOUCH
With the client in a standing grounded position, touch very gently with your middle finger the base of the neck in the occipital foramen, before the first cervical vertebrae. Your hand will be facing down toward the floor.
‘This touch must be done with the conscious intention of activating the innervation of the cranial parasympathetic which innervates the arms, lungs and heart. The aim is to relax the ego control in a way to help the person plunge into his inner being and to get more conscious’ (ibid, p. 57).
It is important for the therapist to note the position of the hands in each touch because they have to be turned toward the same direction of the energy flow (down in both cases) (p. 27–29).
4. SNS Portals
In the SNS branch the muscles of the limbs (to run or fight or reach) and the spine (to mobilize for quick action) are innervated (see SNS nerves toward back (dorsal) part of body in figure 3). This is very familiar to Bioenergetic Analysts who have many techniques to help mobilize blocked affect toward active expression, including kicking, hitting, reaching and expressing emotions, that might be blocked and frozen by the PNS.
5. SNS Portals and Catharsis
Some have argued against catharsis (venting a large build up of emotion) as a viable therapy technique claiming it “floods” the system and that the results are “temporary,” and therefore not valuable. Peter Levine (In an Unspoken Voice) concludes that repeated emotional expression in a cathartic manner (screaming, pounding pillows, etc.) results in release of endorphins, which could be addictive. He touts body awareness over catharsis.
Here is a counter argument from an ANS lens. It is true that under stress, the hyperactive arousal of the SNS can cause acting out of violent aggression from uncontained anger, high levels of agitation, anxiety to a level of panic, and/or fear that overwhelms the person. But in Bioenergetics we show people safe and focused ways to express anger that is not chaotic.
When we use techniques to move the fear or anger through by expressive work, the client does not get stuck in an SNS level. Once they complete a need to express blocked affect, their system feels better and they are no longer flooded. When emotional release happens one automatically moves from the SNS to the SES. They naturally move into the happier, more social SES where the oxytocin and vasopressin (love hormones) contribute to a renewed openness and positive outlook. The new neural pathways for being in the SES are strengthened and can expand the WOT, meaning they feel rewarded for being in the SES zone and the compulsion to act out from the SNS reduces.
In Levine’s view, “There is an addictive quality … that we are drawn to create and re-create” (p. 70). I think he is referring to people (he admits he himself re-created addictive bad relationships) (ibid.) who are organized in hyperarousal and have trouble containing anger. But if one spends more time in the SES, where the whole brain, both thinking and feeling is online, rather than in the SNS, where the compulsion to react to danger by fight or flight is so strong, then the person has more choices. For example, a person feels threatened and gets angry. They feel the impulse to yell at someone they love (in SNS). They take a few breaths, access (strengthened by neural pathways) the SES, use the brain to quickly decide, “I don’t want to hurt anyone” and instead of blowing up they go to the gym to move the anger through. They leave the gym with a flood of endorphins, which makes them feel good in a healthy way.
6. SNS Portal Techniques
a. Grounding
Bioenergetic therapists are trained in observing the energy of the body, including where there is movement and lack of movement in the chronic (usually unconscious) holding patterns of the body. Before activating an expression of fear or anger or reaching that might be blocked, clients are invited to do some form of grounding, which can happen in the relationship (e. g. the therapist making the client feel seen, heard and cared for) and/or internally by opening to the pull of gravity to make one feel centered and therefore have more room for a fuller, more congruent expression. In terms of portals, the SNS is innervated in the dorsal (back) of the body. Grounding helps one feel one’s stance as more grounded. Classic grounding techniques involve rolling the feet over a ball or dowel, leaning on one leg or the other, jumping down, a forward bend, with slow roll up. For detail figures and explanations on classic Bioenergetic techniques see Schroeter and Thomson (2011) Bend Into Shape, Techniques for Bioenergetic Therapists.
b. Activating the SNS
The large muscles, especially the arms and legs are the portals to stimulate active expression (to complete a running away or fighting impulse) from the SNS. This is the realm very familiar to Bioenergetic therapists. From a polyvagal viewpoint, if a client is in the most primitive level, in the stress of the PNS, they could be in danger if they are very depressed or dissociative for an extended time. The danger of staying there too long is to disorganize. If you assess they need to mobilize some aggression, then moving these big muscles could bring energy that moves them into the more energized SNS.
c. Technique
Have a client (after grounding) stomp his/her feet, kick a cube, punch a pillow, hit with a bat or racquet, yell, “No” or other angry sounds. By contrast, if the impulse that needs completion is fear-based, the person can run in place and scream or push away with their arms.
- Case example: I had a five-year-old client who told his mother he was going to “jump out the window and kill myself.” The Mom was distressed because she expected him to be “my happy little boy” even though the boy was upset because the parents were getting a divorce. I brought out a box with wooden balls that had to be hammered vigorously with the wooden mallet to go in the holes. This little boy hammered those balls for 40 minutes! Afterward his Mom reported he could verbalize, “I am mad that you sent Dad away.” When Mom validated his anger, he said, “I love you.”
- PT analysis: This child was in the shock and depression of the PNS, making suicidal threats (jump out of the window). Any input that improves our ability to orient and communicate will inhibit the stress response. By orienting to the present in finding bright colored wooden balls to hit, and by my verbal encouragement the boy moved out of the PNS depressive state. Activating his arms and hands to pound the wooden balls moved him up into the SNS. After that expression was complete (and accepted by Mom) he could move to the SES and verbally express his feelings of both anger and love.
7. Bringing Down Anxiety with the Vagal Brake
The vagal system, according to Porges is a feedback system with motor pathways, sensory pathways and brain pathways to regulate motor output. The vagus nerve acts to inhibit the sympathetics (SNS). Since the SNS is set to run in overdrive all the time (due to our constant scanning for any perceived or real danger), health depends on an active vagal brake. As stated earlier the job of vagal brake is for the SES to stop this constant high level of adrenalized alertness.
Thayer and Lane (2000) as reported in “Cranial Intelligence blog” (Steve Haines, October 4, 2010) show that ANS imbalance (causing anxiety, poor attention and immune disorders …) is due to low vagal tone. This means the vagal brake is not working well. It would be like needing new brake shoes for the car. The vagal brake not working causes the SNS to be disinhibited. Like hitting the car in front of you from behind when your brakes do not stop soon enough, SNS dominance creates disasters to self and often clashes with others. This dominance causes the system to be less flexible in its responses. The following is a Bioenergetic technique to access the vagal brake.
8. SNS Portal Technique to Access the Vagal Brake
To move from the overactive SNS, which is focused externally and innervates the big muscles for action, one needs to activate interoceptive (internal) signals to access the SES. So accessing the heart and the gut are helpful in inhibiting the SNS. We can use the terms “gut brain” or “belly brain” and “heart brain” less as a metaphor and more as a reality, since Porges has shown how the body sends messages afferently from these parts of the body directly to the brain. If the client makes regular use of some type of relaxation and focusing technique, they can grease the wheels so that they can slide more quickly out of the SNS when stuck there. Make sure the vigilant SNS dominated client feels safe before attempting the following Bioenergetic technique:
- Invite the client to close his/her eyes and relax the back by lying down or sitting propped against pillows, where they can feel their back. If SNS flexor muscles are switched on (readiness to strike or move), lying down or relaxing the back sends a signal to the spine, (which is a portal to the SNS), to reduce that flexion. As the client feels his/her back with support, the flexors relax and the more receptive extensor muscles are engaged.
- Next, place your hands (or have the client place his/her hands) on their heart and belly (abdomen) and have them breathe into each area, to observe and relax. The open heart and relaxed belly can inhibit the SNS. Follow the energy to see if they can deepen the breath or have a need to move toward some affect.
9. SES Portals
For the social or communication branch (SES) of the ANS, cranial nerves V, VII, IX, X and XI are the portals. See in figure 3 the nerves going toward the ventral (front) of the body supra (above) the diaphragm and from the neck toward the heart and thus innervating all our expressive and communication modes such as hearing, seeing, speaking and animated emotion. The motor outputs of the SES according to Porges are head turning, muscles of facial expression, muscles of mastication (chewing), middle ear muscles, larynx and pharynx, heart and bronchi. The sensory inputs (portals) to the SES cranial nerves are interoception (from inside, especially heart and gut messages), sound (it changes the tension in the middle ear muscles), mucosal linings of oral, nasal cavities, the sinuses, the teeth and the cranium (skull).
10. SES Techniques
The cranial nerves as a group can be used by gently stimulating their sensory and motor components in the face, throat and neck (Chitty, 2013, p. 137). Here are some examples of using various SES portals. Once open, follow the energy and see if it expands the SES or moves into the PNS (maybe due to a need to cry or grieve) or SNS (due to a need for movement toward expressing fear or anger).
- OPENING THE HEART: Have the client think of someone they love and have them reach toward that person (or a pet). This induces warm feelings and releases the bonding hormones, oxytocin and vasopressin, which are in the SES.
- OPENING THE VOICE: Have the person vocalize words, songs, or emotional expressions. Join them in those sounds if it makes them feel safer or is playful. (Play involves creativity. Interpersonal play expands the SES).
- MAKING FACES: Have the client move the muscles of their face around to loosen facial and eye muscles. Open and close the mouth to loosen the jaw. Next, have them imitate and exaggerate expressions of anger, disgust, worry, fear, anger, sadness, shyness, happiness and joy. Use any variety. If they begin to laugh, this loosens the belly and diaphragm, which is also in the SES.
- MASSAGING THE HEAD OR NECK: The tenth cranial nerve is the origin of the vagus. Any neck massage can stimulate the area. Massage of the skull can calm the hot head of someone stuck in a SNS stress response.
EXAMPLE: I saw the following scene. A woman was spinning in anger and agitated worry, repeating over and over what was bothering her with no resolution. Her husband instinctively went toward her, placed one hand on the back of her head as his other hand covered her forehead and the top of her head. It was almost like a containing helmet. He made a joke, “Heal!” This made her laugh and immediately the overheated spinning monologue dropped away. He looked at her warmly. She smiled back, sharing in his humor and warmth. She had returned to the SES.
D. Summary of PT Implications for Clinicans
- An overall therapeutic goal is to re-establish the Social Engagement System, because it is the most sophisticated in repairing stress. This may occur by completing thwarted movements in the SNS or the PNS.
- If you can identify what state of the ANS the client is currently in, you will have a road map to help him or her.
- It is important to convey to the client that wherever they are in the ANS is adaptive for them.
- Keep in mind that when the newer Social Engagement (SES) fails, then the natural strategy is to go (automatically) to the SNS, if not successful there, then to the PNS.
- Provide clients with a visual of the three branches to help them identify where they are in the ANS.
- Be aware of your voice prosody and facial expression to help invite clients into the SES, where they will feel safest and therefore most cooperative.
- To be the most present as a therapist, you need to be aware of your own ANS state and practice self-care when moving out of the SES.
E. Summary of PT Implications for Somatic Clinicans
- An overall therapeutic goal is to re-establish the SES, i. e., “reclaim a natural, childlike state of joy” (1995, p. 10).
- Identify the current state of ANS using body observations and interpersonal reactions. Is the client in the SNS, SES, or PNS?
- Being stuck in the SNS or PNS means they are feeling threatened and not safe. To shift from stressed PNS or stressed SNS, activate deep breathing. Notice where the energy is stuck.
- Use somatic interventions to help move energy from one state to another.
- Use knowledge of ANS portals to inform your somatic and relational interventions.
- Activate emotional expression to move blocked affect. Grounded anger work mobilizes the SNS. Once discharged, the client naturally moves into social openness of the SES or rests calmly in the PNS. No shift indicates energy is stuck and the client may not feel safe enough to shift levels at this time. Frame this as a protective impulse of neuroception.
- CAUTION: The immobilization of the PNS may be adaptive. Help the client feel safe by mirroring their affect and keeping a safe distance unless invited to help mobilize them. Remind them to orient to the current environment and use it to feel as safe as they can. Helping the client move from the stress response (immobilization) to the normal response (rest and recover) of the PNS may help them recover their balance.
- Become aware of your own signs for moving out of the SES, because the SES is the best level to be in when seeing clients. Valuable self-care techniques are provided in the article, “Bioenergetic Self-Care for Therapists” (Heinrich-Clauer, 2015, BA (25) p. 41–72).
IV. Conclusion
This paper introduced the tenants of polyvagal theory to somatic psychotherapists for the benefit of utilizing the concepts in their clinical work. The concept of neuroception helps therapists appreciate that any action or behavior by a client can be seen as a response to perceived or real danger. Identifying which of the three (SES, SNS, PNS) branches of the ANS the client is in can create a roadmap for interventions. The dissolution from newer to older states helps the therapist understand the neurobiology of affect regulation. Somatic psychotherapists in general and Bioenergetic therapists in particular can use their knowledge of the how the body both expresses and inhibits affect to aid clients in moving through ANS states and expand their capacity for utilizing the SES.
As Pat Ogden writes, “The body speaks clearly to those who know how to listen” (p. 25). While Bioenergetics has always attended to the non-verbal, body-based, implicit processes over verbal explicit processes, polyvagal theory helps us elucidate this language of the body from the point of the nervous system. The body dramatically reveals the three levels of the ANS and shows us visually the shifts between them. Seeing these shifts has always been a nuanced skill from the Bioenergetic toolkit. However, we now have language to label these shifts in a new way. Stephen Porges’ immense contribution to psychophysiological understanding by the introduction of polyvagal theory, gives us a complete map of the ANS. We can now incorporate that map into our clinical understanding and practice.
This paper is an attempt to invite others to ride the wave as it crests. I expect the tipping point to come, where all somatic psychotherapists will easily communicate in ANS terms. This neurophysiological lens aids us in feeling compassion for clients by understanding their behavior in a new light. It can reduce shame in clients by helping them understand their biology from the polyvagal point of view. Incorporating lessons from neuroscience like polyvagal theory into practice strengthens the validity of our work by grounding it in sound science.
References
Berceli, D. (2005) Trauma releasing exercises: revolutionary new method for stress/trauma recovery. Book Surge Publishing.
Chitty, J. (2013), Dancing with yin and yang: ancient wisdom, modern psychotherapy and Randolph Stone’s polarity therapy. Colorado: Polarity Press.
Clauer, J. (2011), Neurobiology and psychological development of grounding and embodiment. Bioenergetic Analysis, (21), 17–55.
Eichhorn, N. (2012), Safety: the preamble for social engagement: interview with Stephen Porges. In Somatic Psychotherapy Today, 1(4).
Heinrich-Clauer, V. (2015). Bioenergetic self-care for therapists. Bioenergetic Analysis 25, 41–72.
Hilton, R. (2008) Relational somatic psychotherapy. M. Seick (Ed.) S. B.Grad.Inst.
Levine, P. (2010), In an unspoken voice: how the body releases trauma and restores goodness. North Atlantic Books.
Lowen, A. (1975), Bioenergetics. New York: Coward, McCann & Geoghen Inc.
Lowen, A. (1995), Joy, surrender to the body and to life. New York: Penguin Books.
Marucheau, L. (2015) Power point for Interpersonal Neurobiology study group
Ogden, Minton, & Pain (2006) Trauma and the body. New York, NY: WW Norton & Company.
Ogden, P. (2013), Sensorimotor psychotherapy: interventions for trauma and attachment. New York: Norton.
Panksepp, J. Biven, L. (2012), The archaeology of mind: neuroevolutionary origins of human emotions. New York: Norton.
Porges, SW. (1995), Orienting in a defensive world: mammalian modifications of our evolutionary heritage. A polyvagal theory. Psychophysiology, 32, 301–318.
Porges, SW. (2011), The polyvagal theory: neurophysiological foundations of emotions, attachment, communication, self-regulation. New York: Norton.
Reich, W. (1933), Character analysis. Vienna: Psychoanalytic Press
Schroeter, V, Thomson, B. (2011), Bend into shape, techniques for bioenergetic therapists. Self-published. Encinitas, CA.
Samsel, M. (n. d.) Shift Toward the Social Engagement System www.reichandlowentherapy.com
Siegel, D. J., Bryson,T. (2011), The whole-brain child. Random House.
Spencer, H. (1864) Principles of biology. New York. Prometheus Books.
Thayler & Lane (2000), in Cranial Intelligence Blog. Haines, S. (10.4.2010).
About the Author
Vincentia Schroeter, PhD, is a licensed psychotherapist in private practice in Escondido, California and on the teaching faculty of the Southern California Institute of Bioenergetic Analysis (SCIBA). She is a member of the IIBA faculty, chief editor of the IIBA journal and co-author with Barbara Thomson of the Bioenergetics techniques manual, Bend Into Shape.
E-mail: vincentiaschroeter@gmail.com