Elements of Comprehending Change-Processes in BA1
From Isolated Self-Regulation to Interactive Regulation: Embodied Resonance (Empathy) and Physical Encounter
Joerg Clauer
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2016 (26), 75–110
https://doi.org/10.30820/0743-4804-2016-26-75 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstracts
English
On behalf of two case studies this paper aims to present some elements in comprehending change-processes of patients suffering from severe disorders. Knowledge of infant research and neurobiology are used as a blueprint for that. Healing processes are considered to take place on the level of implicit embodied relational knowledge – and embodied resonance (empathy), physical cooperation and rhythms to be fundamental elements. Spatiotemporal, affective and bodily proprioceptive forms of communicative exchange – and less the psychodynamic content – are of fundamental importance to self-development of patients in this perspective.
Key words: embodied resonance, fragmented self-experience, mutual developmental process, physical cooperation, “primary triangle”
German
Dieser Artikel versucht anhand zweier Fallgeschichten einige Wirkfaktoren zu identifizieren, die uns helfen können, Veränderungsprozesse bei Patienten mit schweren Störungen/Erkrankungen besser zu verstehen. Dazu werden Erkenntnisse aus der Säuglingsforschung und Neurobiologie herangezogen. Heilungsprozesse würden demzufolge auf der Ebene des implizit-körperlichen Beziehungswissens angestoßen – und Empathie als verkörperter Resonanzprozess sowie körperliche Kooperation und Rhythmen wären fundamentale Bausteine dieser Prozesse. Aus dieser Perspektive betrachtet ist es weniger der psychodynamische Inhalt, der von grundlegender Bedeutung für die Selbstentwicklung von Patienten ist, als vielmehr räumliche, zeitliche, affektive und propriozeptiv-körperliche Formen der Kommunikation.
French
Cet article expose deux situations cliniques dans le but de mieux comprendre les éléments favorables au changement pour les patients qui souffrent de problématiques sévères. Ce sont les connaissances issues des recherches infantiles et de la neurobiologie qui en sont la base. On considère que les capacités relationnelles implicites et somatiques sont au cœur du processus de guérison; la résonnance corporelle (l’empathie), la coopération physique et la rythmicité en sont des composants fondamentaux. Dans cette perspective, pour le développement au niveau du Soi, plus que le contenu psychodynamique, ces sont les interactions et communications spatiotemporelles, affectives et proprioceptives qui seront déterminantes.
Spanish
Por medio de dos estudios de casos, este ensayo tiene como objetivo presentar algunos elementos para entender los procesos de cambio en pacientes que sufren de trastornos graves. Los conocimiento acerca de las investigaciones infantiles y neurobiología se utilizan como un anteproyecto para el mismo. Se considera que los procesos de curación ocurren a un nivel de conocimiento implícito incorporado relacional y de resonancia incorporada (empatía); la cooperación física y los ritmos también son elementos fundamentales. Las formas de intercambio comunicativo espaciotemporal, afectivo y corporal propioceptivo – y menos del contenido psicodinámico – son de fundamental importancia para el desarrollo individual de los pacientes en esta perspectiva.
Portuguese
Tendo por base dois estudos de caso, este artigo visa mostrar alguns elementos para a compreensão dos processos de mudança em pacientes que sofrem de desordens severas. Para isso, utilizamos o conhecimento de pesquisas sobre bebês e da neurobiologia. Considera-se que os processos de cura ocorrem ao nível do conhecimento relacional incorporado implícito, sendo que a ressonância incorporada (empatia), a cooperação física e o ritmo são elementos fundamentais. Formas proprioceptivas corporais, espaço-temporais e afetivas de troca comunicativa são de importância crucial (maior que o conteúdo psicodinâmico) para o auto-desenvolvimento dos pacientes em questão.
1. Introduction
Lowen (1986) described the treatment of psychosomatic illnesses as a difficult task, especially inflammatory diseases of the digestive tract. In 2007, I made some observations in this journal regarding the treatment process of these disorders based on a successful bioenergetic analysis of a patient with ulcerative colitis. In doing so, I not only emphasized the intense transference/counter-transference process but also the particular importance of the three s’s: slowness, safety and support.
This paper now attempts to continue to examine the active processes and facilitating elements of change processes during Bioenergetic long-term treatments. It presents reflections on the relevance of empathy (embodied resonance) and bodily cooperation in the therapeutic process of patients with “early disorders.” “Early disorders” are not only disorders of vitality affects or vitality dynamics (cf. Stern, 1986/2011) but primarily self-loss experiences or fragmentations, i. e. the loss of the cohesion of self-experience. Orange, Atwood and Stolorow (1997, p. 47f.) have differentiated the following self-loss experiences:
- Psychic fragmentation: the experience of psychological selfhood disintegrates into parts
- Somatic fragmentation: the unity and integrity of the experience of your body is lost
- Psychosomatic fragmentation: your body and mind are experienced as irrevocably separated.
In the case studies two patients tried to preserve their own threatened self in various ways:
- A patient with a psychosomatic fragmentation and his desperate attempt to control his surroundings as much as possible for the safety of his own self-experience.
- A second patient suffered from mental and somatic fragmentations with disturbances to her basal vitality dynamics combined with a helpless, resignative abandonment of her self-assertion.
Sander (2009, p. 163) said that self-psychology must turn to two areas in order to understand the ontogenesis of behavior and psychological organization: early childhood development and biology (that is today neurobiology too). This also corresponds to the understanding of bioenergetic body psychotherapy.
The present IIBA-website uses in explaining Bioenergetic Analysis a statement of Robert Lewis about body and words: “we listen to the inner resonance – of your inchoate secrets – as it lives in your body … but we also listen carefully to your words and are touched by them when they come from a depth no one can put a hand on.” Lewis (2000, 2004, 2005) himself like Resneck-Sannes (2002, 2012) and many others have presented case stories and attempts to understand the importance of attunement and resonance or bodily interaction as elements for change processes in Bioenergetic analysis and psychotherapies. In even more detail the “Boston Change Process Study Group” for about two decades already is occupied with investigating change processes in psychotherapies (Stern et al., 2010). They have a background of psychoanalysis and infant research with a paradigm of research that focuses on the attunement in the mother-infant-dyad mainly via exteroceptive channels i. e. vision and hearing. This misses mostly a focus that is important for Bioenergetic Analysis, a more systemic point of view that integrates the father (Fivaz-Depeursinge & Carboz-Warnery, 2001) and the bodily sensorial channels of touch, proprioception and tactile sensations.
This paper tries to integrate some of those points of view in understanding change processes in the presented cases of Bioenergetic therapies. Special attention is thereby paid to embodied resonance (empathy) and bodily cooperation in the therapeutic relational dialogue which is considered as a mutual developmental process within the patient-therapist dyad. Before I describe the cases, I will first direct my attention to early childhood development and (neuro-)biology in order to create a framework for the comprehension and comments on the case histories.
2. Early Childhood Development
2.1. Empathy and Dyadic Affect Attunement
Empathy is the basis for attunement processes between the infant and mother or other caregivers at the beginning of life already and, therefore, also for the beneficial self-development of the baby (cf. Schwaber, 2013, p. 98). Sander understood the coordinated interaction between mother and infant as a resonance between two systems (cited by Schore, 2005, p. 403). Winnicott (1974) had already pointed out that the mother and infant only exist as a system, and that there is no baby without the mother and vice versa. Both are dependent on each other in their biological regulation. One example is breastfeeding. It is of vital importance to the diet of the infant and can be vital to the mother after childbirth since it helps her uterus to regress and can counteract bleeding and infection. Otherwise, the self-regulatory skills of the mother could be overwhelmed and she would have to depend on medical assistance.
This interdependence is obviously significantly greater for the baby. Its immature system needs the regulating aids of the mother, particularly after birth, not only in order to survive and to maintain physical homeostasis, but also to stimulate the baby and to regulate and dampen any stress states and over-excitation. In terms of its sleep-wake rhythms and instable vegetative regulation of its temperature for example, the infant is largely dependent on the empathetic, contingent regulatory care of a caregiver. This is made easier by a – hormonally mediated – particularly pronounced empathy of the mother towards her infant (cf. Ammaniti & Trentini, 2009). According to Stern (1992), all these processes can be assigned to the phase of the emerging sense of self. The infant does not internalize the object or partial objects, but rather the process of mutual regulation (Stern et al., 2012).
Sander (2009) not only described important organizing principles for these somatopsychic attunement processes like the principle of specificity, but in particular the principle of rhythmicity and the agency of the individual. Moreover, he formulated the following phases of problems in the development of the mother-infant system (month of life = ML):
| 1. Primary regulation of biological processes (for homeostasis) | 1st–3rd ML |
| 2. Reciprocally coordinated exchange of physical activities | 4th–6th ML |
| 3. Initiative of child’s activities | 7th–9th ML |
| 4. Focus on the availability and limits of the mother | 10th–13th ML |
| 5. Self-assertion in opposition to the mother | 14th–20th ML |
| 6. Recognition (awareness, expression+ regard of intentions) | 18th–36th ML |
| 7. Continuity (recognition +cohesion of a differentiated self) | 18th–36th ML |
I also mention Stern’s developmental stages of a sense of self here. Important to me are the evolving and prevailing forms of “NO” in these phases of a sense of self, which I will employ together with Sander’s phases, to comment on these case histories. They are a central part in the development of the infant’s emancipation just as much as the development of patients with disorders in their self-experience and are summarized in figure 1.
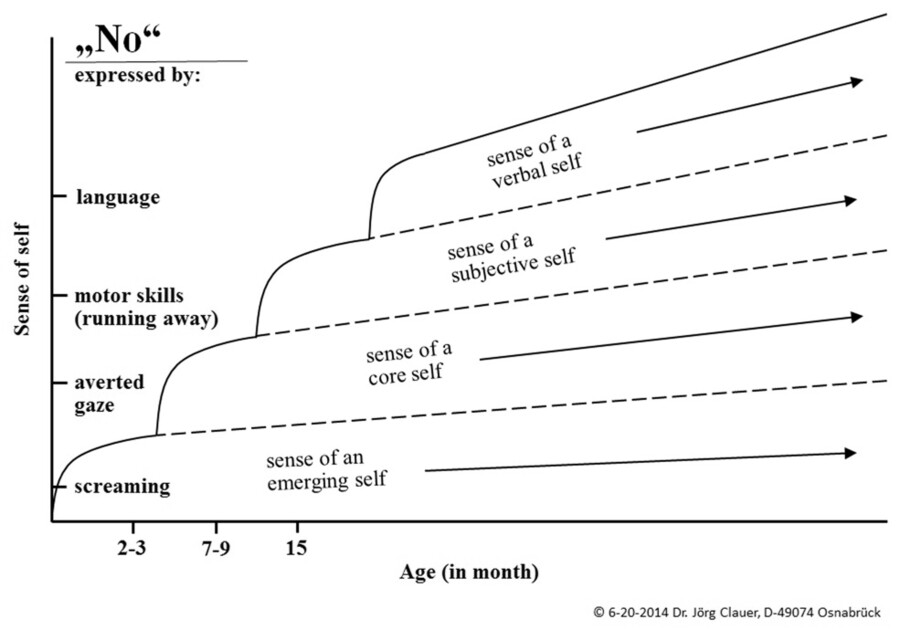
Figure 1. Developmental phases of the sense of self and delimitation, of saying “NO” (according to Stern, 1986)
In vitally important process of breastfeeding we already can observe two essential interactive regulatory processes within the dyad. One channel of communication was frequently more the focus of the attention of researchers. It primarily involves eye contact, facial expressions and the exchange of affects, e. g. during playful moments after breastfeeding. The second channel of bodily-cooperative attunement is a separate dynamic developmental trajectory that receives a great deal of attention in body psychotherapies and that also includes contact and skin contact. For a long time, this second area received little attention in the research on the mother-child dyad (however, see e. g. Beebe et al., 2010, 2014).
2.2. From the Dyad to the Triad: Cooperation and Physical Principles of Organization
Triangulation has particular status in the theory and thinking of psychoanalysis and its resulting methods such as bioenergetic analysis. In practice, however, analytical psychotherapy, including self-psychological methods and BA, were primarily concerned with disorders of affective exchange, bonding and mentalization processes. Neurobiology and infant research had likewise focused on affect attunement for a long time. At least from a physical standpoint, all these perspectives primarily deal with processes within a rather distanced dyad.
It was only the systemic perspective inspired research on the “primary triangle” – the playful interaction of infant, mother and father – by Fivaz-Depeursinge and Carboz-Warnery (2001), Fivaz-Depeursinge and colleagues (2010) and by von Klitzing (2002) for example, that shifted bodily attunement processes more into the focus of infant research. It shows how, starting from birth, family cooperation by the parents promotes infant development. The infant is actively seeking joint/triadic communication. So-called family alliances, i. e. cooperation in the family, require the involvement of all three members. This involvement and relational attunement can, as in the dyad, become easily disturbed. If the parents’ ability to cooperate is disturbed, then the triad disintegrates into dyads or monads. Restoring (or securing) this cooperation is, according to the research, dependent on certain physical organizational patterns between the three family members (cf. Clauer, 2009a, 2011, 2013a,b,c). This was already evident in the developmental stage of the body-core self (in two to three-month-old infants) and is based on four physical interaction levels, which are linked to corresponding mental functions:
- Pelvis = participation: the orientation of the lower body towards one another is fundamental and crucial as to whether or not all three partners in the relationship are involved in the interplay (basal rootedness of social interactions, turns towards the partner).
- Torsos = organization: the relation of the upper body (shoulders) indicates whether or not each partner is aware of his/her role (leans towards the partner at the appropriate distance).
- Gazes = focus of attention: the position of the head (direction of gaze) indicates whether or not all three partners are able to create a shared focus of attention.
- Facial expression + voice = affective contact: expressive behavior indicates (similar to dyadic play) whether or not each partner is able to initiate, develop and maintain affective contact and thus emotional intimacy.
When playing in the triad, the respective partners must therefore attune themselves to different physical levels. The critical involvement of all participants for a shared joyful game first of all depends on the physical orientation of pelvis and legs to each other. Without the physical attunement from orientation by turning towards the other person with the lower body and without the affection by leaning forward with the upper body at a reasonable distance, no common focus of attention can be created by the coordination of gaze directions, and no mimical affect attunement can arise as well. Metaphorically speaking, affect attunement, like the tip of the iceberg, cannot appear above the surface of perception if the interaction between the physical attunements – like the main part of the iceberg – did not exist below the water’s surface.
It should be mentioned that the research of Beebe and Lachmann on interactive regulation in the dyad work just as early in the 2nd –3rd ML and with the same paradigm of joy in shared play as the “primary triangle” research. In the meantime, Beebe and colleagues (2010, 2014) also report that not only the rhythms of gaze sequences but the patterns of contact and touch (and thus skin contact) as well within a mother-child dyad at 4 months of age can also help to predict either a secure or a disorganized attachment at the age of one year. The dynamic developmental trajectory of bodily collaboration or co-operation in the further course of development in infants has been researched by Downing (2006, 2007). He refers to the process of the rhythms of physical dialogue in connection with the rhythms of affective exchange as “micro-practices.” How both developmental trajectories unfold their effect and significance together is depicted in the studies conducted by Tomasello (2009). He describes mimical and gestural-physical attunements as the basis for the development of symbol formation and language. Accordingly, it is in the “primary triangle” that we first begin to anchor ourselves in our first social community/group, namely within the family. This is the beginning of growing into our culture, our language and into our higher cognitive functions. Tomasello (2009) speaks of the formation of a common (social) experiential background – a “common ground.”
2.3. Primary Triangle and the Oedipus Myth
The research on the primary familial triangle has shown us that the entire family and their cooperation are important. Affect attunement thereby proves to be rooted in physical attunement. As early as during or even before pregnancy, the preconceptions of parents about their future joint care for their infant can be used to predict their later real cooperation and hence how the developmental fate of their yet unborn child will look like (cf. Klitzing, 2002). This is reminiscent of the Oracle of Delphi who predicted the fate of the not yet conceived Oedipus to his parents. According to this view, it is not the ancient gods (or drives) who determine2 the tragic fate of a person in advance. It is rather the type of relationships, the affection, cooperation and empathy of the parents for their infant that determine a person’s developmental fate.
When we take a look at the Oedipus myth (Schwab, 2008) in this light, then the instinct-driven internal conflicts and repressions in the soul of a man are not the most important aspects here in my opinion. Rather, the myth describes the tragic pre-oedipal, early childhood developmental fate of Oedipus as a result of the lack of love and cooperation between his parents. According to the bodily organizational principles as we find them described in the primary triangle, the early trauma of Oedipus in the myth is represented by his pierced feet (Clauer, 2011). This is pure symbolism without any comprehensible real need. To kill a young infant, it is enough to abandon it, as in the Oedipus saga, to a wild mountain landscape. From a bioenergetic-analytical point of view, however, I see this as a symbol of how the early trauma prevents the adult Oedipus from being well anchored or grounded in his own bodily self-experience, in his emotions and in his relationships, thus as his inability to stand on the ground of reality, which is characterized by social relationships. This social ground of reality Oedipus had problems to recognize clearly in the myth and we might say that his social intelligence had not developed well. This is symbolized by the fact that he put himself to blindness. The trauma and impairment to his development from the lack of loving cooperation and coordination between his parents in the myth eventually leads to the hateful-impetuous nature of Oedipus – this does not result in a mental malformation of instinct-driven fates.
2.4. Empathy, Affect Attunement and Physical Coordination in Psychotherapy
Besides introspection, it is empathy that has been emphasized by self-psychology as a central factor of psychotherapy. Self-psychology most often assumes that observing a face and facial expressions will reveal the inner life of a person (cf. Milch, 2001), as also suggested by the work of Krause (1983) and Darwin (1872). However, the trialogue game reveals that without the physical attunement from an orientation by turning towards the other person with the lower body and affection by leaning forward with the upper body at a reasonable distance, a common focus of attention cannot be achieved by coordinating gaze directions and facial attunement. This does not become immediately apparent in dyadic infant research and is taken for granted. This creates the false impression that the entire attunement and development process solely occurs by mimical affect attunement alone. Recent research, in contrast, shows that we can meaningfully decipher facial signals only in the overall context of the significance of physical signals (Aviezer et al., 2012; Herrmann, 2012). This is comparable to the fact that all the sensory signals from our large sensory organs, like our eyes and ears, only receive meaning within the context of proprioception together with tactile and vestibular sensations (i. e. the body’s inner signals) and especially within the context of physical motion signals (Clauer, 2009a). This also means that the physical movements and signals of the entire body are more important for the attunement processes in our relationships than is often assumed (cf. Clauer, 2013b).
The interactions and attunement sequences between mother and infant are first of all a process on the implicit-procedural level. Feelings and posture patterns can also be conveyed in the psychotherapeutic treatment situation via the physical resonance processes of empathy, the embodied countertransference. I understand empathy in terms of sensitivity towards and feeling into the other person as a process of physical co-vibration or a coming into resonance with the non-conscious reality and the feelings of another person (Clauer, 2003; Heinrich, 1997; Heinrich-Clauer, 2008, Lewis, 2005). Psychoanalytic authors often emphasize the cognitive components of empathy (e. g. Barwinski, 2014). Empathy is described as a complex process that not only involves affect resonance but also a perspective assumption as prosocial behavior and cognitive processes of comprehending interpreting (Milch, 2001; Kilian & Köhler, 2013). As a Bioenergetic analyst, I emphasize corporal-emotional resonance as the implicit-procedural root of empathy. For about 15 years, I have explored the processes of an empathy understood as embodied resonance and of embodied countertransference (cf e. g. Clauer & Heinrich, 1999; Clauer, 2003, 2008, 2009a, 2013b, c).
According to Schore (2005, 2011), the cerebral processing of these embodied exchange processes is lateralized in the right brain and is predominant in the first one and a half to two years of an infant’s life. Similarly, the right hemisphere is also ascribed a functional dominance in regulating the autonomous (organ) functions and the primary emotions (Porges, 2010, p. 76). The transmission of implicit knowledge and relationship knowledge from one person to another was also referred to by Schore (2005, 2011) as communication from the right side to the right side of the brain.
Mindfulness training for the implicit bodily processes – such as Bioenergetic analyst training – therefore makes it easier for therapists to understand how the patient is doing, how he is feeling. An empathic attitude is determined by a constant attentiveness to the embodied relationship statements. The facial expressions, gestures, posture, eye expressions, voice and breathing rhythms of the therapist and patient influence one another (cf. Zaccagnini, 2008). Less intersubjectively described but similarly, Koehler says that feelings which cannot be verbally transmitted are introduced into therapeutic situations by acting out, by facial expressions, movements, motoric restlessness and physical reactions such as sweating, palpitations and dizziness (cf. Milch, 2001, p. 283). The work of Rizzolatti (1999) and others have validated the respective motoric, sensory and affective processes (Bastiaansen et al., 2009) with mirror neurons and a process of embodied simulation, the model of the “embodied simulation” (Gallese, 2009). In the end, this means that a psychobiologically attuned therapist can become the interactive regulator of the experiential world of his patient (cf. Tonella, 2008, p. 64).
Beebe and Lachmann (2002, p. 35, 143f.) described key points that are of crucial importance to both dyadic and triadic attunement processes and for adult psychotherapy3 as well:
- Ongoing intertwined nonverbal (and verbal) patterns of self-regulation and interactive regulation.
- Interruption and restoration of ongoing regulations.
- Increased affective moments.
These principles apply to both verbal and non-verbal regulatory paths. Regulation is organized according to these principles and the internalization of these kinds of patterns of experience is co-created.
The processes and organizational principles of embodied resonance are the basis for the exchange and interactive regulation between parents and infant not only. They are for sure the basis for access to early, implicit unconscious personality traits and disorders in the cohesion of self-experience to arise within the therapist-patient interaction too.
Embodied resonance can ultimately be consciously understood in the mutual therapy process. This most often is an integrative achievement by the therapist to understand these processes in a decryptive manner (to decipher them) and, if necessary, to reflect them verbally – the empathic insight can but must not be symbolized and verbally formulated (cf. Lyons-Ruth, 1999)! This kind of understanding shifts the focus and importance from the psycho-dynamic contents to the interactive (bodily) forms and types of communicative exchange within psychotherapies. The interactive forms of communicative exchange will be a focus of my observations in the case studies.
3. The Neurobiological Perspective
3.1. Self-Perception and Consciousness
To neurobiologist Damasio (2000, 2011) and to Metzinger (2005, 2009), self-perception/emerging sense of self, primal emotions, consciousness and spirit do not primarily arise as a function of the cerebral cortex: “Although the cerebral cortex is an important part of this system, I believe the brainstem to be the foundation of the self-process” (Damasio, 2011, p. 206). The received afferent information from the body, particularly the interoceptive information that is transmitted via the vagus from the internal organs, lead – based on the brain stem – to a proto sense of self that is associated with background feelings/vitality affects. The proto self emerges as a product of the integration of multiple sensory body perceptions, especially from the inner milieu of the bodily fluids and organs, the tactile sense of the skin, kinesthetic signals of the musculoskeletal system and the vestibular organ. This integration is in many ways “susceptible to interference,” especially in the brainstem (ibid., p. 265). “The self is incrementally constructed on the foundation of the proto self” (ibid., p. 34). The information of our body system as a whole is therefore closely linked to our vitality affects and is the basis of the development of consciousness and a sense of self. In turn, the described vitality affects remind us of the important vitality contours in infant development by Stern (1986, 2011).
Only the change of the proto-self by interaction with objects can give rise to the pulses of a core self-perception that is capable of consciousness. Self-perception and consciousness are therefore tied to an interaction, the exchange with objects or persons. This model thus confirms self-psychological/intersubjective perspectives in which the patient and therapist unavoidably influence each other and co-create their conscious experience. Fragmentations and other self-experience disturbances are thus distinguished by the fact that the joint interactions and attunement processes are disturbed and must be restored. In the case of psychosomatic fragmentations it seems to me that a retreat into a forced self-regulation caused by developmental trauma takes place for the sake of ensuring the survival. However, an existential achievement of mammals no longer comes into play: the chances of survival and the welfare of mammals improve considerably from life and attunement in the group.
Self-perception and affects are thus inextricably tied to interactions, and without movement, no meaningful information can arise from our sensorial perceptions of the world. Only the internal or external movement of a vital, vibrant body leads to the perception and consciousness of a coherent self in its relatedness to the environment. A withdrawal from environmental stimuli soon leads to a fragmentation of self-experience. The rootedness in our bodily self-perception thus determines how we find our way in the world, how we navigate it (Damasio, 2000, 2011). The movements and impressions of our body form the basis for our sense of self. When this physical anchor is lost, we also lose the coherence/integration of the self (-experience). Winnicott (1974, p. 193f.) already provides similar approaches:
“The true self comes from the vitality of the body tissues and the activities of bodily functions, including the heart’s activity and breathing. […] The true self appears as soon as there is any mental organization of the individual whatsoever, and it means little more than the totality of sensomotoric vitality.”
It should be noted that self-perception and conscious self-awareness is inextricably tied to basic experience of affects. In treating psychosomatic patients it is also important to know that the emerging self-perception/sense of self and affective experience is intertwined with the vegetative regulation via the vagus complex i. e. the autonomic nervous system (ANS), at the brain stem level. Moreover, the vagus complex, i. e. the vagus and other cranial nerves4, are also involved in regulating the mimic facial muscles and the muscles for swallowing, phonation and hearing.
In this way, the emerging self-experience (and consciousness) is coupled with basal affects and the facial expression on the brainstem level, and it is closely tied to the vital-vegetative regulation of the functions of our internal organs and with social interaction. Figure 2 attempts to depict relevant nuclei in the brainstem for that, but not connections to other brain areas relevant for a more complex sense of self.
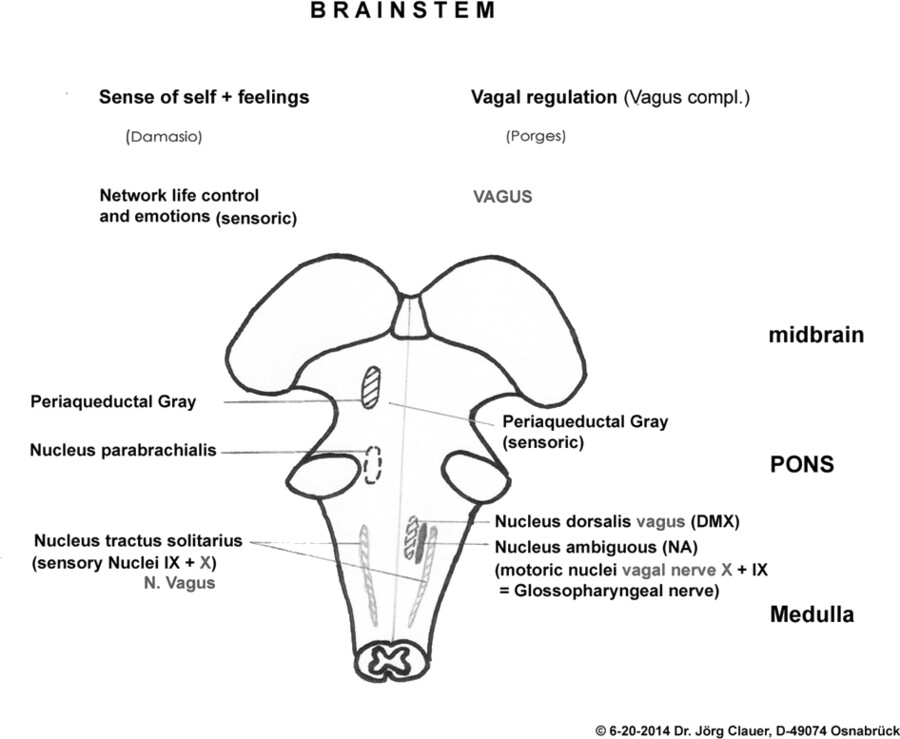
Figure 2. Brainstem © 6/20/2014. (according to Ferner & Staubesand, 1973; Porges, 2010; Damasio, 2011)
3.2. Prosocial Ventral Vagus Complex(VVC).
Porges’ (2010) Polyvagal Theory differentiated the vagus in such a way that we can no longer assume the duality of a sympathetic and parasympathetic nervous system today, but rather a tripartite autonomic nervous system (ANS) as depicted in figure 3. In doing so, Porges employs the concept of neuroception and thus refers to an unconscious, continuously-vigilant scanning of the safety situation in our social environment.
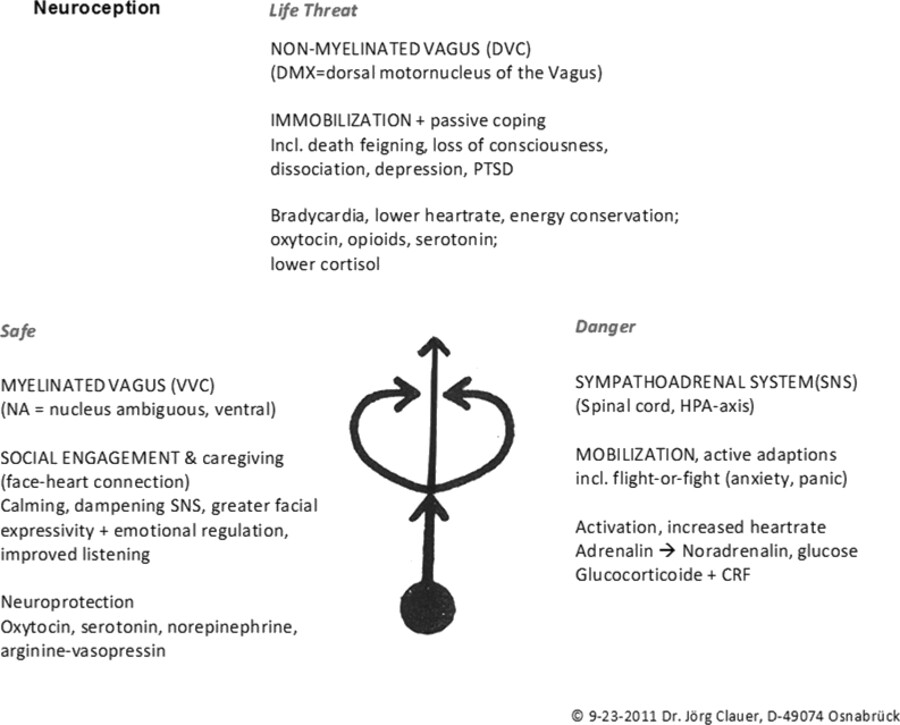
Figure 3. Tripartite autonomic nervous system (ANS) © 9/23/2011. (according to Porges, 2010; Reich, 1972), presented at the 21st International Conference for Bioenergetic Analysis in San Diego/California
A psycho-vegetative situation to a moderate level of arousal and a trusting sense of safety is controlled by the ventral vagal complex (VVC) in the brainstem. This ventral vagal complex (VVC) is comprised of a myelinated vagus part from a ventral original core, the nucleus ambigus (NA), and cores of the trigeminus and facial nerves. The VVC is clearly related to the expression and experience of emotions (ibid., p. 77). When operating in its environmental perception of safety mode, it employs its so-called VAGAL BRAKE to inhibit an increased level of arousal and the mobilizing flight and fight readiness of the sympathetic nervous system (ibid., e. g. p. 249). Under the influence of the vagal brake, the dorsal vagal core (DVC) in turn stimulates the regenerative digestive processes during safe, resting situations. But when it is intensely stimulated under existentially threatening situations as the ventral vagal brake is released, the dorsal vagal core (DVC) then controls immobilizing, constrictive or dissociative reactions during life-threatening situations. Besides shock-induced paralysis, it can then engender pathological phenomena such as stomach ulcers, intestinal inflammation or sleep disorders. The ability of social engagement (“System Social Engagement,” ibid., p. 174f.) that is connected to VVC-function depends on how we influence our facial and cranial muscles with the aid of neural pathways that connect the cortex and the brainstem (the cortico-bulbar pathways). These muscles make our face expressive and allow us to communicate meanings by gestures, to influence the sound of our voice, to turn our gaze to certain things and to distinguish human voices from background noise with our hearing. If the ventral vagus complex is constricted during a situation that is experienced as potentially life-threatening, then the neural regulation of the mimical facial muscles and cranial muscles, and thus perception and affective expression, are impaired as is often the case in psychosomatic illnesses such as alexithymia. Alexithymia refers to the inability to perceive or to read feelings. Bioenergetic analysts see a link here to the concept of “cephalic shock” as introduced by Robert Lewis (2008).
3.3. Psychotherapeutic Consequences
In summary, empathy with the bodily experiences and emotions of the infant (or the patient) establishes the ground or secure basis for the development of his/her self-awareness and self-esteem. To establish a sense of safety for the infant through interactive regulation also always means to regulate fear, anger and over-excitation. This follows a pattern: the child leads – the mother follows (cf. Schore, 2005).
If the environment is not attuned, hostile or insufficiently sensitive and non-empathetic in terms of cooperation during infancy, then impairments or trauma may result. Corresponding repetitive violations of empathy from withdrawal by the caregiver and abandonment or by not corrected/restored misattunements lead to hyper- or hypoarousal and, in time, to mental and anatomically tangible changes. The absent sense of safety in the relationship, which corresponds to a lack of secure attachment or experience of a reliable self-object, leads to a loss of trust in interactive regulation, and can lead to a retreat into a forced self-regulation and/or the urge and attempt to control the hostile experienced environment/reference persons as comprehensively as possible. This can easily go along with hyperarousal and fight or flight reactions, as we will see in my first case description. If the attempt at interactive control fails, then fragmentation reactions, a sense of powerlessness and devitalization can arise, as in the second case description.
Even if disturbed patients with early developmental traumas frequently have a pronounced desire for human empathy, understanding and backing or support, they exhibit a lack of confidence and security in the human group. Porges describes something similar in his model of neuroception and emphasizes that early disturbed patients with developmental trauma in particular easily misinterpret the attentiveness and attention of a psychotherapist on the subconscious level. Even the friendly facial expressions, voice or benevolent attitude of the therapist often seems not to reassure. His proximity is experienced as a threat or even as an existential threat. With this core idea, Porges (2010), in line with trauma therapists like van der Kolk, concludes that dialogical and especially verbal psychotherapy not only do not reach these kinds of patients, but even harms them and could retraumatize them. Porges thus recommends music therapy as the method of choice.
Thus he points to the fact that resonance and attunement to rhythmic bodily experiences like music can be helpful for those patients in particular. In addition to a support in this way, my experience is that disorders incurred in relationships need to be cured in relationships finally. Yet, as therapists of these kinds of patients we find ourselves in a situation that I compare with the image of an iceberg.5 On the explicit level of conscious awareness and in the verbal dialogue of the talking cure, we are predominantly aware of the small proportion of the patient’s self that is visible above the water. With our bioenergetic-analytical radar systems, we try to infer the large proportion under water, the implicit, embodied experience area, the implicit relational knowledge (cf. Clauer, 2013b). However, in the icy regions of people with a severely wounded self-experience we always run the risk of running aground with our own implicit-procedural, unconscious portion under water and of sinking on a traumatized patient iceberg that was shock-frozen in its early experience. That means to fail as a self-object and not being able to restore relatedness and attunement after inevitable breaches of the interaction.
For this to happen less frequently, all dialogical psychotherapies like bioenergetic analysis and self-psychology, according to my experience, provide a great opportunity to not only incorporate empathy and empathic affect attunement but psychotherapeutic collaboration/cooperation as well and thus the entire (potential) space of implicit-procedural processes within the therapeutic relationship. The collaborative attunement processes are not only the basis of body psychotherapeutic ways of working. Its importance was also emphasized by Lyons-Ruth (1999, cited from Lachmann, 2010 p. 93f.) that
“systems of meaning are organized to capture implicit or procedural forms of knowledge. Enactive processes can be better articulated and integrated by participating in more coherent and collaborative forms of intersubjective interaction. In order to promote therapeutic care, these enactive processes do not necessarily need to be translated into reflexive symbolic knowledge or verbalized. The collaborative process, which incorporates the dialogue between patient and analyst as much as enactments do, helps to foster its ‘implicit relational knowledge.’”
I want to demonstrate how this may look like based on the following two case descriptions. In the first case of a patient with a predominantly psychosomatic fragmentation, the main focus is on the security of self-experience and existence by controlling the therapeutic situation or scene. In the second case of a patient with a complex fragmentation, the main focus is on collaboration and rhythmic bodily attunement processes. Both patients have suffered a variety of traumas in their life histories.
4. Case Histories
4.1. 1st Case: A Psychosomatic Case History – from the Self-Regulating Organ Mode to the Interactive Mode
When the patient came to me at about 39 years of age, his ulcerative colitis had flared up massively after conflicts with his male boss. He took cortisone and azathioprine, an immunosuppressant used for intestinal inflammation. A behavioral therapy had proven ineffective.
The parents were very young when he was born and quarrelsome. They did not cooperate and had no loving relationship. They were only sporadically present. Often he was at his discontented grandmother together with his younger sister. According to this background, to protect him from his violent father, he was sent by his mother and grandmother between the age 10 and 17 to a Catholic boarding school where he was sexually abused by a priest. Exhibiting an open bisexual orientation, he is married and has two daughters.
4.1.1. On the Course of Therapy: A Painstaking Birth – Reviving Mutual Regulation
Phase 1: Adapting Yourself to the Patient
As a sign of his alexithymia, the patient could not communicate anything about his anxiety and other emotions. Instead, he repeatedly spoke of an inner emptiness. At the end of the therapy he said: “The most difficult part for me was to perceive my actual affectivity and emotional equilibrium. Until now, I had to control my environment with great vigilance and keep a look out for any escape routes. This minimized the danger that my fears would attack my gut in milliseconds.” His constant readiness to fight was intended to prevent him from experiencing himself completely at the mercy in relationships, of losing control and self-regulation and that it “went right into his pants,” as he said and this caused him tremendous shame. To achieve a sense of safety whenever he found himself in new surroundings, he had to first find out where the nearest toilet was.
Right away he had a strong urge to control the time frame and spatial organization of our setting. Particularly in the initial phase of the therapy did he insist on frequent, even longer “work-related” interruptions of our therapy sessions. I was only able to achieve certain continuity in the therapy sessions by reacting very flexibly to his scheduling demands. He himself quickly remembered the story of Oedipus and threatened me indirectly with something similar to the fate of that father: in case of any dispute over the arrangement of the relationship, he would cut me out of his life by discontinuing the therapy. I often found it hard to overcome my anger about being coerced in such a way and every now and then called into question the controlling nature of the relationship arrangement. Sometimes I needed my supervisor in order not to try to employ “gentle force” on my part to urge the patient to do something like an extension of the therapy which he considered to be long superfluous. Only after a period of almost three years did he also succeeded in recalling positive experiences with his father and said: “Instead of hate mongering, I frequently have compassion for my father now.”
To avoid being other-directed again, the patient frequently exhibited no attunement with me as regards the change of speaker. I then had the feeling, with my impulses to say something, of standing opposite a tightly woven curtain of his uninterrupted flow of words that seemed to spill out at me like the wall of a waterfall. I felt other-directed again in the course of this scenario and had the impression that my feeling was probably something similar to what the patient had felt in his own childhood.
We initially sat diagonally opposite each other. Later on, after some experiments with the setting, he selected a spot at a right angle, laterally removed on the therapy mat. He often looked straight ahead in that position and not at me. Here, too, I registered a “rumbling” in my belly after some period of time. I addressed this in a playful manner at some point, and also started to look straight ahead. In doing so, I cast doubt on the one sided interactive regulation. He was extremely irritated by this and protested vehemently. He wanted my continuous undivided attention (with the option that only he could look away). However, the question regarding how he had experienced the situation and me and the enquiry into our interaction led to a restoration of the attunement and made the reciprocity of the attunement more conscious.
Besides the aforementioned averted gaze, running away was also an important relationship regulation for him. Whenever he became overexcited, he would abruptly run to the bathroom. I felt some empathy for his somatic-vegetative need and the threat of shame in remembering a time of dysentery in my life. My benevolently communicated acceptance of this “regulation” was important to him in order that he experienced himself as understood and accepted, as he related to me. Beside that it was hard work for me to accept him rejecting all exercises and physical contact offered by me. Even during colitis flare ups he refused any soothing physical contact (a kind of contact I used in a former case of ulcerative colitis; Clauer, 2008). This provoked feelings of being helpless and impotent as a Bioenergetic Analyst. He also continuously rejected all other physical interactions and also avoided any expression of emotion. But through the body psychotherapeutic endeavors, he clearly realized that any notion of physical proximity to me was tied to a fear of losing control, of helplessness and the expectation of a great threat.
Phase 2: Proximity and Emotional Neglect
A major turning point came after almost two years and from an entirely surprising incidence to both of us. Just before my vacation, I went to see a doctor and unexpectedly met the patient there early in the morning. We were alone in the waiting room. I was puzzled and felt insecure how to react with a kind of tightness. For sure I greeted him and then sat down at some distance, but inevitably at a right angle to him, like in our therapeutic setting. It was an uncomfortable ambivalent situation. The unexpected proximity led to an acute episode of his ulcerative colitis.
After my vacation, he told about the first outbreak of his illness for the first time. He succeeded to be expelled from boarding school by stealing and then lived at his grandmother’s. Yet his attempt to graduate from high school failed. After his subsequent civilian service, he stayed in the Holstein area, apprenticed there as a plumber and lived with his first girlfriend. He remembered that he had felt completely uprooted after finally moving out of his parents’, who he vehemently rejected. The parents of the girlfriend, in contrast, showed kind feelings to him. It was during this time in his apprenticeship and with his girlfriend that the disease now broke out. The desire at that time for a secure relationship regulation and a secure bond were hardly reconcilable with the fear of a loss of autonomy and self-regulation.
After the encounter in the doctor’s waiting room, he also arrived to the next session after my vacation with a dream that best captured his affliction. In the dream, he discovered a corpse embedded in concrete in the floor of a hidden basement room. The description was so vivid as if we were both standing together in this basement room. For the first time, he also described a feeling, namely: “to be emotionally encased in concrete.”
Phase 3: Coordinated Activities and the Thawing of Emotional Worlds
In my next vacation a few weeks later I had hiked over the Alps. Directly upon our first greeting, he inquired about my vacation experience. Contrary to my analytical habit and surprise, I gave him a spontaneous, direct, authentic response. After this response, he developed the image of us on a joint Alpine hike and of using me as a scout on his path.
During the course of our hike, we encountered – like in his dream – a frozen corpse in the ice, an “Ötzi,” or iceman. He now experienced the process of a slow physical and emotional thawing connected to the emerging memories of his experiences of abuse. We understood our surprising proximity in the doctor’s waiting room as the trigger for his remembered experiences of abuse. In the further course of his treatment, he took advantage of opportunities to also process the abuse via the court system.
I can also remember situations on our joint hike where tears, which the patient could not yet cry, came to my eyes when I experienced empathy with him emotionally abandoned and lonely in the Catholic boarding school for instance. He seemed to notice this and later reported that he was now able to weep at home with his wife following any moving or emotional therapy process. At the end of the therapy we then experienced that he could cry tears in my presence.
Phase 4: Opening the Door for Mutual Regulation
The common experiences in the therapy process and during the imaginary hike had led to a secure experience basis. Our attention now turned to a social third party – the escalating conflict with his boss. He experienced her to be as possessive as his mother was, felt emotionally abused, and fought a long, tough and fierce battle with her. Contrary to my fears, the changes achieved so far remained stable.
After quitting and receiving his severance pay, this dispute finally ends one year later. What remained was an issue which he described using a picture from a book: a “porte recondamnée,” i. e. a safety door like the kind used in the food industry, which can only be opened from the inside with a horizontal handlebar. His solitary anguished self-regulation as a safeguard against his feeling of being threatened by his surroundings had now received a handy (and great) symbolization in the truest sense of the word. In this last phase of the therapy he could finally allow to be emotionally touched as well, allow tears and bodily contact and feel compassion for his father. He tried his best to meet my available appointment dates. In his desire for a sense of solidarity, he was able to open the symbolic, one-sided inner door and allow moments of powerlessness and helplessness.
I was particularly pleased by the fact that his gastroenterologist had diagnosed a healthy intestine during a colonoscopy 6 months prior to the end of his therapy. This finding also persisted without the need for any additional medication. Our farewell after the long hike was moving for both of us.
4.1.2. Commentary on the Therapy Process
According to Sander as well as Beebe and Lachmann, temporal, spatial and affective attunements and joint (movement) rhythms are effective organizational principles of communication throughout life. When we transfer Sander’s descriptions of problems in the development of the mother-infant dyad onto the therapist-patient dyad, some similarities can be found for the aforementioned therapy process.
The first phase of therapy, however, can be understood as a covert struggle over access to an interactive regulation. The patient exhibited at different levels a great effort to control the time frame and the spatial organization of our settings. My first response or countertransference to this scenario, with the angry feelings, corresponded to his implicit and then also verbally stated experience and threat of an oedipal struggle for power and dominance with me as the therapist-father. I also found this very pronounced in his one-sided and often lacking temporal attunement regarding the change of speaker. It is known that this kind of lack of attunement triggers very aversive feelings that I myself could not escape from. Had I primarily let myself into this fight mode and not contained or processed/digested this ire, then the patient would have terminated the relationship/therapy as he threatened to do.
The initial phase can also be understood and regarded in a different way. He had described that his parents were young, overwhelmed and at odds with each other. So there was not much loving cooperation between them or much affection for him. As in my alternative assessment of the Oedipus myth (cf. 2.3.), it is obvious that the patient was disturbed/traumatized early on in his self-development. The organ mode of his colitis can thus be seen as a (controlled by the dorsal vagus) shameful emergency response to a threat. The patient tried to prevent its occurrence by a forced control of his environment. The nature of this “vegetative relationship regulation” can be compared to Sander’s 1st phase of the primary regulation of biological processes for maintaining homeostasis. Like the mother who must attune herself to her baby in the first phase of life, I felt prompted by him at the beginning of our work process to largely adjust my practice organization to his temporal, spatial, physical and affective rhythms (according to the “child leads, mother follows” formula). If a mother does not adjust herself to the needs of her infant so that it then experiences itself as neglected, other-directed, overwhelmed or threatened, then the baby is only left with an inner withdrawal from the relationship with his unsuccessful protest. Similarly, the patient repeatedly expressed that the therapeutic relationship would be interrupted or aborted should I not adapt myself to his “needs.” Like mothers experience it from time to time, I sometimes developed a distinct reluctance or annoyance at the efforts involved in making these adjustments. The importance of implicit nonverbal cooperative path of relational attunement processes in the psychotherapy of “difficult patients” on the levels of temporal patterns, spatial relatedness, affective arousal and physically-proprioceptive stimulation have also been pointed out by Kiersky and Beebe (1994, p. 390). A similar position can be found in Massimo Ammaniti (2009), who points to the importance of physical attunement processes in psychotherapeutic processes.
My mostly adequate adjustment to his needs had paved the way for changes and developments in the relationship. His influence on our relationship formation gradually fostered a sense of safety in the relationship and a feeling of participation as well as authorship and agency – in place of the fear of his overwhelming helplessness and powerlessness. I regard his initiative to select another spot as a sign of increasing security. This selection had given him new ways of regulating eye contact and attention in our working relationship. It was now easier for him to either isolate himself or to turn towards me. This ensured his participation in the relationship regulation. It was in his hands to direct his attention/turn towards me and he was able to further unfold a feeling of self-efficacy(agency)/authorship instead of powerlessness with the no of his averted gaze.
All in all, this therapy phase again and again showed indications and elements of Sander’s descriptions of phases 2 + 3 regarding the development of reciprocal exchange and the initiative of the child (cf. Sander, 2009 p. 318f.). In particular, the reciprocal rhythmic relatedness with gaze aversion is identified by Sander as part of the reciprocal exchange of physical activities. My averted gaze put into question the rather one-sided interactive regulation in which he led and I followed. When we examined his protest of my averted gaze, this returned my attention back to him and gave me a little more room to play in as a step towards greater perceived reciprocal regulation. The negotiation over boundaries and influence in the relationship continued to foster a sense of security, self-confidence and, above all, his own self-efficacy/authorship. My interventions like my gaze aversion can be compared to “Ferenczi’s active technique” (2004). They enabled an unfolding of interactive regulation processes in the therapeutic dyad during the further course of the treatment which were reminiscent of Sander’s problems 5–7 (cf. chapter 2.1.).
A respective phase-specific potential embodied “NO” is of great importance to the development of agency and autonomy. Fig. 1 tries to show phase specific differences of a “NO” in that way. In the beginning, he had threatened me with the complete break-up of the relationship – similar to how an infant may initially do so with a complete inward retreat in the form of “glassy eyes” whenever his cries (also known as a cry baby) show no practical success (cf. Stern, 1986). In addition to the exhibited “NO by gaze aversion,” he still exhibited the “motoric NO by running away” to the bathroom. These interactions can be seen as stages of a development towards autonomy. Only much later, during the period of his struggle with his female boss, was the “verbal mode of NO” at the focus of his development.
At the beginning of our mutual process, the patient quickly felt himself at the mercy of the situation. His subsequent description of the constant watchful control of his environment in this phase of the therapy is reminiscent of Porges’ (2010) description of neuroception. My experience of the relationship and his subsequent descriptions suggest that he found himself in a constant fight and flight readiness when scanning his surroundings and thereby neurovegetatively in a state of SNS hyperarousal. Any movement that came too close to him and questioned his control of the social environment (i. e. with his boss as he often reported and the therapist as well) immediately triggered a reaction that matched a regulation by the dorsal vagus (DVC). He quickly experienced himself existentially threatened and his gut took control of regulating (proximity and) distance in a relationship with these diarrheal attacks. I myself experienced an ambivalence to stay at a distance he was able to tolerate and an impulse to offer to him a soothing bodily dialogue or “empathic contact” especially in times of his colitis flare ups (as I knew it to be effective from a former case of ulcerative colitis, Clauer, 2008). This relational problem Porges maybe addresses in his neurobiological understanding. His proposal to intervene with music therapy might have been another way to soothe the relational tension I felt and towards a solution of the intersubjective problems.
In our case we took another way. The unconsciously initiated and controlled early developmental processes described by the patient were then followed by the surprising situation in the doctor’s waiting room with his resulting reaction in the organ mode, a colitis flare-up. His unexpected inquiry about my vacation experiences allowed him, unlike in the doctor’s waiting room, to re-establish the initiative and control. When I opened myself up to his question and spontaneously gave him an authentic response and thus relinquished my boundaries and control, could he then risk the joint Alpine hike. He could now use me as a scout, as he said, as a useful self-object. In his conception of the mountain hike, it was a first confirmation that we were on our way to establish a physical cooperation and mutual affect regulation. This is reminiscent of Sander’s 3rd and 4th initiative phases (which already occurred when he selected the seated position) and the focus on my availability and limitations as relationship partner during our long, imagined mountain hike. Even emergent memories of abuse and the thawing of his emotional shock-induced paralysis were now possible, which – also viewed with the neuroception model – appears as a confirmation of the increasing social security within our relationship. Witnessing my expressions of emotion like my tears, probably also helped the patient out of his emotional freeze. Naming feelings was certainly not decisive in this alexithymia patient. He benefited much more from witnessing my expressions of emotion which reflected his incommunicable or not perceived emotions. The shared experiences during the (imaginary) hike also created, considering Tomasello’s (2009) work, the shared basis for a common language of emotion and compassion, and thus a change in his alexithymia.
In the last therapy phase while struggling with his female boss, the issues of Sander’s phases 5–7 emerged even more than in our direct interaction. It was a tough struggle for his self-assertion in opposition to the boss (phase 5). In doing so, he took advantage of the resulting security in his relationship to me in terms of a backing for an early triangulation. He also struggled for the (consciously experienced) attention of his intentions and the recognition of his delimited self. So it is understandable that he definitely experienced his termination of employment and separation as progress. He also regarded it as a step that confirmed his position and boundaries. It also concerned developmental issues which Sander refers to as recognition and continuity, as phase 6 and 7.
The patient thus felt sufficiently secure with me at the end of the hike during the time of the dispute with his boss – which was by the way a triangulated situation. This way it was possible that, despite the threatening and tense situations, his old patterns of SNS hyperarousal were no longer transferred into his customary shock frozen immobilization and the associated organ mode of the colitis regulated by the dorsal vagus (DVC), but could be regulated together socially and then increasingly abated.
4.2. 2nd Case: Bodily Cooperation and Psycho-Vegetative Regulation
4.2.1. Symptoms and Case History
This 44 year-old patient who was living alone came to psychotherapy with a severe recurrent depression with a morning low. Even as an adult, the woman who was often traumatized in childhood was accustomed to calming herself with jactitation, that is, with rocking motions. These self-reassurances were not enough to calm her down when her job situation aggravated. This came about by excessive demands, but especially by devaluating comments which threatened her unstable self-esteem again and again. Even hospital stays could not prevent further decompensations/autonomic dysfunctions. Since no more sleep function was eventually recorded at the sleep laboratory, she was forced into early retirement. An important resource to her were her singing skills, which she employed while playing in a women’s cabaret up to her retirement.
She came with an evening medication of 125 mg of TAXILAN, 50mg of opipramol, promethazine (atosil) as needed and a 2 x 40 mg beta-blocker due to a hyperkinetic heart syndrome since the age of 18. A preceding bioenergetic psychotherapy and equine-facilitated therapy with my wife had enabled her to start psychotherapy with me as a male.
She grew up poor as the third of five children and the only girl. The parents suffered from alcohol dependency, attacked each other with knives and beat their children. The mother was particularly unfair. The children had to watch the father rape their mother. The only positive experience in her life was probably her living near grandmother. She had also won judo championships in her childhood which the father had encouraged until puberty. She said, “I functioned in life, finished school and my apprenticeship and have always worked. But I’ve very much still remained a child and never let myself in on sexuality. Since a longtime boyfriend betrayed me with my best girlfriend, I hold on tightly to my alcohol and cigarettes and withdraw myself from the world entirely.”
4.2.2. The Course of Therapy: Coordinated Physical Cooperation
In the first few months she learned how to use the balance-disc, the Do-In (a structured self-massage that promotes the cohesion of self-experience and mindfulness: (cf. Clauer, 2009a, b; Kushi, 1994) and became familiar with and used for herself the safe internal place and vault for traumatized individuals. But none of these things led to any significant, lasting changes in her behavior or symptoms. Her inner experience only reorganized itself within our embodied relationship dialogue. We worked using rhythmic movements sitting back to back on a Pezziball (a gym-ball of a diameter of 50–80 cm), or I held her head and moved it gently back and forth while she lay on the therapy mat. As time went by she repeatedly requested this type of cooperation and nevertheless was so full of fear that her eyebrows vibrated and both our breath got caught mostly in the beginning when I held her head. As I grounded myself in my ischium-bones and relaxed my breathing she was able to relax slowly too more and more.
After many or, more specifically, more than one hundred “experiments” back to back or by holding and rhythmically moving her head, she became increasing relaxed in the therapy. Only now did she relate her periodic immersion in the parallel worlds of her girlhood dreams and about the true amount of her alcohol consumption.
4.2.3. Initiative and Self-Efficacy
She followed my intended movements on the Pezziball or relinquished her head to my hands for a long time. In doing so, she had adapted herself to my lead. Eventually she surprised me by saying that my predominant left-right movements on the ball were different from her own rocking – and she initiated back and forth movements. She talked about her sensations during the “experiments” and became more and more active. Out of her isolated, almost autistic seeming self-regulation via the jactitation came cooperative regulation and mutual attunement.
4.2.4. Dreams – Access to the Unconscious
She would now regularly bring her dreams to the session. An intense dream- analytical process developed that accompanied the body psychotherapeutic work, which later faded into the background. Her interest was now focused on our discussions about her dreams. She was pleasantly surprised by the, to her, new interest in the world of her inner experience and my response to it. She was increasingly fascinated by the joint journey into the often frightening world of her dreams in which she no longer felt alone now. In these dreams she was on the run6 down the branching corridors, passageways and shafts of a menacing labyrinth, most of the time some vague subjects behind her. She was usually without orientation, found no way out and would finally wake up in cold sweat. This scenery and the process essentially stayed this way for a long period of time. But she now was able to share her hopeless experience with me and remembered similar feelings and the burdensome experience in her childhood and family.
It was a dense process of empathic sharing of experiences that she was until now completely isolated with, similar to her jactitation. Often I felt some tightness in my chest, my breath got caught again, it was too threatening and no way to scream and I had a sensation of being lost in space. Mostly I was busy to keep my breathing alive and to investigate and understand her dream situation in comparison with her life situation and her remembered childhood experience – and all in all to find with her some hope and confidence in change. I thereby overlooked almost a fundamental transformation that already took place: she was able to sleep again and therefore retain her dreams and bring these along with her. The physical fragmentations were thus abating. With further advances in the therapy, the dreams finally transformed: they became “brighter,” with more and more orientation and finally with exits and ways out.
4.2.5. Vitality and Sexuality
In the further course of the therapy she could now also address her problems with sexuality. She stopped the alcohol abuse and reduced the medication to finally 50 mg TAXILAN besides the beta-blockers. Her sleep behavior was also improved under the reduced medication. She felt more agile and more alert during the day, mingled with people again, earned money for singing lessons and performed with a singing group. She found back to her own voice and rhythm after our reenacted rhythmic encounter. Finally, she met a partner with whom she “got to know sexuality as something enriching” for the first time in her life as she remarked. She has since married, resumed her work and is struggling to find solutions to the problems of her partner’s sons.
Only at the end of the therapy did she finally told me that she had experienced herself in the figures of various famous men on a regular basis at the beginning of our collaboration – in terms of a multiple personality. These psychic fragmentations had disappeared according to her accounts at the beginning of her romantic relationship.
4.3. Comments on the 2nd Case History
The patient initially reported how she had learned to merely function in life and thus increasingly reported indirectly about her “false self.” Her symptoms pointed to very basal “proximal” disturbances of vitality, self-awareness and self-regulation with effects on the vegetative level of the ANS with heart arrhythmia and sleep deprivation. This was tied to a great distrust of men and relationship, which corresponds to an impairment in the “Social Engagement System” in the neuroception model (see chapter 3.2.). The hyperkinetic heart syndrome is, according to Porges (2010), a clear indication of a chronic hyperarousal of SNS. Her traumatized psychobiological system was geared to a variety of potential risks. In light of a constantly experienced (or inwardly feared) threat, it is an adaptive response that the vagal brake and the mode of social trust were only very difficult to reactivate (cf. ibid., p. 251). The in her childhood multiply traumatized patient was accustomed to calming herself with jactitation, that is with rocking motions, even as an adult because she had not experienced calming experiences in relationships to a sufficient extent. The thus necessary self-reassurances from cradling or swinging movements are one of the most effective strategies of vagal stimulation and reactivation of the vagal brake (ibid., p. 233). But even these self-calming measures were insufficient when the situation escalated at her job. The excessive demands and especially the devaluations threatened the coherence of her fragile self and harmed it over and over again. Her existentially threatened self-experience was then left only to reactions controlled by the dorsal vagus (DVC) like hypoarausal with dissociations and a vegetative collapse with a lack of sleep, with panic and depression.
If we now follow Sander’s (2009, cf. 2.1) developmental stages, then the self-experience and self-regulation of the patient as a truly “early disorder” were disturbed down into the first basal level of biological regulation. This was connected to the consequences as described by Schore (2005, 2011) and Porges (2010) of chronic hyperarousal (hyperkinetic heart syndrome) or eventually the symptoms of a controlled hypoarousal via the DVC. Since rocking motions are supposed to be very effective in stimulating the vagus, it is no wonder that the rhythmic attunement and action processes on the Pezziball or when holding and moving the head turned out to be particularly helpful. In a similar manner, parents soothe their infant with rocking movements in early infant development. According to Sander, these can be compared to the second phase of his classification and regarded as a reciprocally coordinated exchange of physical activities. They are also reminiscent of the protoconversations of Colwyn Trevarthen (2009) and the formation of repetitive patterns, i. e. of RIGs as described by Stern (1986). With the rhythmic movements, new repetitive patterns, new experiences of security and relaxation emerged within the therapeutic relationship in the course of our “one hundred experiments.” This was a sufficiently secure basis for her impulses and communicated desires to find an affirmative response. It eventually led to a qualitative envelope where initiative and self-efficacy of the patient in the relationship to the therapist were able to develop and express themselves and received an inner self-confidence. This corresponds to Sander’s phases three and four.
Likewise in Porges’ (2010) preferred music therapy rhythmic processes exist that he says to be beneficial. In working with this patient, however, it were rhythmic bodily-cooperative attunements within a dyadic therapeutic relationship which had changed the regulation in the ANS in terms of a neuroception of safety and thus a reactivated vagal brake (Porges, 2010). As we see rhythmic processes in music therapy seem to be a valuable, helpful instrument in psychotherapy as well as rhythmic bodily processes within an embodied relational dialogue. The resulting sense of safety in the relationship can also reconcile or explain improved sleep and social activities with the neurobiological findings.
The process of rhythmic attunement and cooperation involved constant searching and was accompanied with feelings of great insecurity in me over a long period of time: afraid to either overwhelm her and conjur up catastrophic results or give in to a regressive maelstrom and sink into or get bogged down in it with the patient because – in addition to her desire for physical interaction – she regularly stressed that she would never work again. My analytic superego accused me of wish fulfillment and of complying with her regressive pursuit for amends. However, in time I understood her desire never to work again as a progressive, self-protecting attitude and differentiation from the devaluations at her job that had harmed her self-coherence and had triggered the decompensations. The patient herself had repeatedly very clearly expressed how beneficial our work was to her and that she only feared the curtailment of treatment by her health insurance. She had therefore been content with a frequency of only 2 hours a week.
The actively-induced action dialogues have therefore not, as often feared by psychoanalysts, constricted or even prevented the room for play, imagination and symbolization. On the contrary, the bodily experiences promoted new prosocial behavioral possibilities and opened up space for dream analysis and symbolization. Conflicts, for example regarding dependency versus autonomy, were thus made accessible to processing. Her new capacity for love thus proved to be a confirmatory expression and the result of this conversion and developmental process.
5. Conclusion
Employing the two dynamic trajectories of infant development can be of great value in psychotherapies of patients suffering from severe disorders or fragmentations of self. Those two are affect attunement that builds on the second one, the physical cooperation and relational rhythms. Self-awareness, affects and consciousness are tied to movement and interaction, the exchange with objects or persons. The rootedness in our bodily self-perception thus determines how we find our way in the world, how we navigate it. When this physical anchor is lost, we also lose the coherence/integration of the self (-experience). A withdrawal from environmental stimuli soon leads to a fragmentation of self-experience.
Comparable to the parent-infant interaction the temporal, spatial, affective and bodily proprioceptive forms of communicative modes of exchange and rhythms are of fundamental importance for the self-development of patients. They are the background for a process-oriented Bioenergetic analysis. The leading edge in this way is the embodied resonance (empathy) and bodily cooperation in the therapeutic dialogue which is considered as a mutual developmental process of the patient-therapist dyad. Similar to the situation of mother and baby we sometimes need to give into the patient leading the relational process. Like in the first case history all our exercises and bodily contact offered might be refused then. Nevertheless it is of great value to be in contact and resonate to patients with the full range of our embodied relational knowledge and an empathic attitude that is determined by a constant attentiveness to the embodied relationship statements. In the second case study we notice, according to the work of Porges, that regular rhythmic modes of bodily relational dialogues similar as music are of special value to change processes of patients with trauma and fragmentations.
This kind of comprehension shifts the focus from psycho-dynamic contents to the interactive (bodily) forms and types of communicative exchange within psychotherapies. The implicit nonverbal path of relational attunement and rhythms of cooperative bodily regulations are effective organizational principles of communication throughout life and in psychotherapy of “difficult patients” as well. They are for sure the basis for access to early, implicit unconscious personality traits and disorders in the cohesion of self-experience to arise within the therapist-patient interaction too. To establish understanding for attunement and developmental processes within a therapeutic dialogue can promote the healing process in this perspective.
Footnotes
- [1]
- Extended version of a lecture that was held at the 1st Maschsee Symposium in Hanover, Germany in June 2014 and was tied to a co-lecture by Franz Herberth. I thank the Maschsee Working Group whose work and discussions are a constant source of rich suggestions. I am particularly grateful to my colleague Franz Herberth for his vital, cooperative-stimulating and respectful cooperation.
- [2]
- The topic of a predetermined fate or of aspirations and actions as a point of view has become topical again from the discussion of a neurobiologically influenced determinism.
- [3]
- I have also addressed the significance of these attunement principles in my psychoanalytic dissertation: Clauer, J. (2007): Anyone who shows emotions has lost. On the co-construction of healing rhythms in analytical psychotherapy of a patient with structural problems.
- [4]
- The vagus and other cranial nerves (such as the trigeminal, facial, glossopharyngeal nerves) are tied with evolutionary developments from the branchial arch.
- [5]
- The image of the iceberg is familiar to me from a paper by Shapiro (2000).
- [6]
- The impersonal pressure, excessive demands and lack of appreciation at her place of work in a spacious building were, besides being abandoned by her boyfriend and girlfriend, the main triggering factor for her decompensations.
References
Ammaniti, M. (2009): Reply to Commentaries. Psychoanalytic Dialogues, 19, 585–587.
Ammaniti, M. & Trentini, C. (2009): How New Knowledge about Parenting Reveals the Neurobiological Implications of Intersubjectivity: A Conceptual Synthesis of Recent Research. Psychoanalytic Dialogues, 19, 537–555.
Aviezer, H.; Trope, Y. & Todorov, A. (2012): Body Cues, not Facial Expressions Discriminate between Intense Positive and Negative Emotions. Science, 338, 1225–1229.
Barwinski, R. (2014): Differenzierung der Gegenübertragung anhand entwicklungspsychologischer Konzepte. Psyche, 68, 517–536.
Bastiaansen, J. A. C. J.; Thioux, M.; Keysers, C. (2009) Evidence for mirror systems in emotions. Phil. Trans. R. Soc. B., 364, 2391–2404.
Beebe, B. & Lachmann, F. M. (2002): Infant Research and Adult Treatment: co-constructing interactions. Hillsdale, NJ, The Analytic Press. German: (2004): Säuglingsforschung und die Psychotherapie Erwachsener. Stuttgart: Klett-Cotta.
Beebe, B.; Jaffe, J.; Markese, S.; Buck, K.; Chen, H.; Cohen, P.; Bahrick, L.; Feldstein, S.; Andrews, H. (2010): The origins of 12-month attachment: A microanalysis of 4-month mother-infant interaction. Attachment and Human Development, 12, 1–135.
Beebe, B. & Lachmann, F. M. (2014): The Origins of Attachment: Infant Research and Adult Treatment. New York: Routledge.
Buti-Zaccagnini, G. (2008): Affektive Beziehungen und Körperprozesse. In: Heinrich-Clauer, V. (Hg): Handbuch Bioenergetische Analyse. Gießen, Psychosozial: 151–160. Engl. (2011): Affective Relationships and Bodily Processes. In: Heinrich-Clauer, V. (Ed): Handbook Bioenergetic Analysis. Gießen: Psychosozial-Verlag, 149–158.
Clauer, J. (2003): Von der projektiven Identifikation zur verkörperten Gegenübertragung: Eine Psychotherapie mit Leib und Seele. Psychother. Forum, 11, 92–100.
Clauer, J. (2008): Verkörpertes (leiblich-seelisches) Begreifen: Die Behandlung psychosomatischer Erkrankungen in der Bioenergetischen Analyse. In: Heinrich-Clauer, V. (Ed.): Handbuch Bioenergetische Analyse. Gießen, Psychosozial: 383–409. English: (2011): Embodied Comprehension: Treatment of Psychosomatic Disorders in Bioenergetic Analysis. In: Heinrich-Clauer, V. (Ed): Handbook Bioenergetic Analysis. Gießen: Psychosozial-Verlag, 369–394.
Clauer, J. (2009a): Zum Grounding-Konzept der Bioenergetischen Analyse: Neurobiologische und entwicklungspsychologische Grundlagen. Psychoanalyse & Körper 15(2): 79–102. English: (2011): Neurobiology and Psycholgical Development of Grounding and Embodiment. Bioenergetic Analysis, 21, 33–42.
Clauer, J. (2009b): Balancierscheibe und Baumübung. In: Fliegel, S. & Kämmerer, A. (Ed.): Psychotherapeutische Schätze II. Tübingen: dgvt-Verlag, 29–30.
Clauer, J. (2011): Kooperation in der Entwicklung des Menschen 1: Implikationen für die Bioenergetische Analyse. 2: Die Füße des Ödipus in neuen Schuhen. Forum Bioenergetische Analyse, 1, 42–89.
Clauer, J. (2013a): Psychovegetative Regulation, Kooperation, Triade und das Grounding-Konzept der Bioenergetischen Analyse. Thielen M (Ed.) Körper-Gruppe-Gesellschaft. Gießen: Psychosozial-Verlag, 277–286.
Clauer, J. (2013b): Die implizite Dimension in der Psychotherapie. In: Geißler, P.& Sassenfeld, A.(Hg): Jenseits von Sprache und Denken. Implizite Dimensionen im psychotherapeutischen Geschehen. Gießen: Psychosozial-Verlag, 135–173.
Clauer, J. (2013c): Das verkörperte Selbst: Empathie und Embodiment. körper – tanz – bewegung, 1, 13–20.
Clauer, J. & Heinrich, V. (1999) Körperpsychotherapeutische Ansätze in der Behandlung traumatisierter Patienten: Körper, Trauma und Seelenlandschaften. Zwischen Berührung und Abstinenz. Psychother Forum, 7, 75–93.
Damasio, A. R. (2000): Ich fühle, also bin ich. Berlin, List. Engl. (1999): The Feeling of what Happens. Body and Emotion in the Making of Consciousness. New York: Harcourt Brace & Company.
Damasio, A. R. (2011): Selbst ist der Mensch. München, Siedler. Engl. (2010): Self comes to Mind. Constructing the Conscious Brain. New York: Pantheon Books.
Darwin, C. (1872): The Expressions of the Emotions in Man and Animals. London, HarperCollinsPubl. German: (2000): Der Ausdruck der Gemütsbewegungen bei dem Menschen und den Tieren. Frankfurt/M.: Eichborn.
Downing, G. (2006): Frühkindlicher Affektaustausch und dessen Beziehung zum Körper. In: Marlock, G. & Weiss, H. (Eds.): Handbuch der Körperpsychotherapie. Stuttgart: Schattauer, 333–361.
Downing, G. (2007): Unbehagliche Anfänge: Wie man Psychotherapie mit schwierigen Patienten in Gang setzen kann. In: Geißler, P. & Heisterkamp, G. (Eds.): Psychoanalyse der Lebensbewegungen. Wien: Springer, 555–581.
Ferenczi, S. (2004): Schriften zur Psychoanalyse II. Gießen, Psychosozial.
Ferner, H.; Staubesand, J. (1973): Sobotta/Becher: Atlas der Anatomie des Menschen, Band 3. München: Urban & Schwarzenberg.
Fivaz-Depeursinge, E. & Corboz-Warnery, A. (2001): Das primäre Dreieck. Heidelberg, Carl-Auer. Engl. (1999): The Primary Triangle. New York: Basic Books.
Fivaz-Depeursinge, E., Lavanchy-Scaiola, C., Favez, N. (2010): The Young Infant’s Triangular Communication in the Family: Access to Threesome Intersubjectivity? Conceptual Considerations and Case Illustrations. Psychoanalytic Dialogues, 20, 125–140
Gallese, V. (2009): Mirror Neurons, Embodied Simulation, and the Neural Basis of Social Identification. Psychoanalytic Dialogues, 19, 519–536.
Heinrich, V. (1997): Körperliche Phänomene der Gegenübertragung – Therapeuten als Resonanzkörper. Forum der Bioenergetischen Analyse, 1/97, 32–41. Engl. (1999): Physical Phenomena of Countertransference: Therapists as Resonance Body. Bioenergetic Analysis, 10(2), 19–31.
Heinrich-Clauer, V. (2008): Therapeuten als Resonanzkörper: Welche Saiten geraten in Schwingung. In: Heinrich-Clauer, V. (Ed.): Handbuch Bioenergetische Analyse. Gießen: Psychosozial-Verlag, 161–178. Engl. (2011): Therapists as Resonance Body. Which Strings come into Action? In: Heinrich-Clauer, V. (Ed): Handbook Bioenergetic Analysis. Gießen: Psychosozial-Verlag, 149–158.
Herrmann, S. (2012): Nebulöse Mimik. Süddeutsche Zeitung, 277, 18.
Kilian, H. & Köhler, L. (2013): Von der Selbsterhaltung zur Selbstachtung. Gießen: Psychosozial-Verlag.
Kiersky, S. & Beebe, B. (1994): The Reconstruction of Early Nonverbal Relatedness in the Treatment of Difficult Patients: A Special Form of Empathy. Psychoanalytic Dialogues, 4(3): 389–408.
Klitzing, K. von (2002): Frühe Entwicklung im Längsschnitt: Von der Beziehungswelt der Eltern zur Vorstellungswelt des Kindes. Psyche, 56, 863–887.
Krause, R. (1983): Zur Onto- und Phylogenese des Affektsystems und ihrer Beziehungen zu psychischen Störungen. Psyche, 37, 1016–1043.
Kushi, M. (1994): Do-In-Buch: Übungen zur körperlichen und geistigen Entwicklung. Holthausen: Mahajiva.
Lachmann, F. M. (2010): Heimkehren – Going Home. Selbstpsychologie, 39, 86–101.
Lachmann, F. M. (2012): Säuglingsforschung und die Behandlung Erwachsener. Selbstpsychologie, 47, 7–18.
Lewis, R. (2000): Trauma and the Body. Bioenergetic Analysis, 11/2, 61–75.
Lewis, R. (2004): Projective Identification Revisited – Listening with the Limbic System. Bioenergetic Analysis, 14/1, 57–73.
Lewis, R. (2005): The Anatomy of Empathy. Bioenergetic Analysis, 15, 9–31.
Lewis, R. (2008): Der Cephale Schock als Somatisches Verbindungsglied zur Persönlichkeit des Falschen Selbst. In: Heinrich-Clauer, V. (Ed.): Handbuch Bioenergetische Analyse. Gießen: Psychosozial-Verlag, 113–128. Engl.(2011): Cephalic Shock as a Somatic Link to the False Self Personality. In: Heinrich-Clauer, V. (Ed.): Handbook Bioenergetic Analysis. Gießen: Psychosozial-Verlag, 113–127.
Lyons-Ruth, K. (1999): The two-person unconscious: Intersubjective dialogue, enactive relational representation, and the emergence of new forms of relational organization. Psychoanalytic Inquiry, 19, 576–617.
Metzinger, T. (2005): Die Selbstmodell-Theorie der Subjektivität: Eine Kurzdarstellung in sechs Schritten. In: Herrmann, C. S.; Pauen, M.; Rieger, J. W. & Schicktanz, S. (Eds.): Bewusstsein: Philosophie, Neurowissenschaften, Ethik. München: UTB/Fink, 5–32.
Metzinger, T. (2009): Der Ego Tunnel. Berlin Verlag, Berlin. Engl. (2009): The Ego Tunnel. The Science of Mind and the Myth of the Self. New York: Basic Books.
Milch, W. (2001): Lehrbuch der Selbstpsychologie. Stuttgart: Kohlhammer.
Orange, D.; Atwood, G. & Stolorow, R. (1997): Working Intersubjectively: Contextualism in Psychoanalytic Practice. Hillsdale, NJ: The Analytic Press. German: (2001) Intersubjektivität in der Psychoanalyse: Kontextualismus in der psychoanalytischen Praxis. Frankfurt/M.: Brandes & Apsel.
Porges, S. W. (2010): Die Polyvagal-Theorie. Paderborn, Junfermann. Engl. (2011): The Polyvagal Theory. New York: W. W. Norton.
Reich, W. (1972): Die Funktion des Orgasmus. Frankfurt/M.: Fischer. (Orginalausgabe [1942]: The Function of the Orgasm. Orgone Institute Press).
Resnick-Sannes, H. (2002): Psychobiology of Affects: Implications for a Somatic Psychotherapy. Bioenergetic Analysis, 13/1, 111–121.
Resnick-Sannes, H. (2012): Neuroscience, Attachment and Love. Bioenergetic Analysis, 22, 9–28.
Rizzolatti, G.; Fadiga, L.; Fogassi, L., & Gallese, V. (1999): Resonance behaviors and mirror neurons. Archives Italiennes de Biologie, 137, 85–100.
Sander, L. W. (2009): Die Entwicklung des Säuglings, das Werden der Person und die Entstehung des Bewusstseins. Stuttgart: Klett-Cotta. Engl. (2008): Living Systems, Evolving Consciousness, and the Emerging Person. Hillsdale, NJ: The Analytic Press.
Schore, A. (2005): Erkenntnisfortschritte in Neuropsychoanalyse, Bindungstheorie und Traumaforschung: Implikationen für die Selbstpsychologie. Selbstpsychologie, 6, 395–446. Engl. (2002): Advances in Neuropsychoanalysis, Attachment Theory and Trauma Research: Implications for Self-Psychology. Psychoanalytic Inquiry, 22, 433–484.
Schore, A. (2011): The Right Brain Implicit Self Lies at the Core of Psychoanalysis. Psychoanalytic Dialogues, 21: 55–74.
Schwab, G. (2008) Die schönsten Sagen des klassischen Altertums. Frankfurt/M.: Fischer Tb.
Schwaber, E. A. (2013): Empathie: Eine Form analytischen Zuhörens. Selbstpsychologie, 49, 80–108.
Shapiro, B. (2000): Will Iceberg Sink Titanic. Bioenergetic Analysis, 11/1: 33–42.
Stern, D. N. (1992): Die Lebenserfahrung des Säuglings. Stuttgart: Klett-Cotta. Engl. (1986): The Interpersonal World of the Infants. New York: Basic Books.
Stern, D. N. (2011): Ausdrucksformen der Vitalität. Frankfurt/M., Brandes & Apsel. Engl. (2010): Forms of Vitality: Exploring Dynamic Experience in Psychology, the Arts, Psychotherapy and Development. Oxford: Oxford University Press.
Stern, D. N. et.al. (The Boston Change Study Group) (2012): Veränderungsprozesse. Frankfurt/M.: Brandes & Apsel. Engl: (2010): Change in Psychotherapy. A Unifying Paradigm. New York: W. W. Norton.
Tomasello, M. (2009): Die Ursprünge der menschlichen Kommunikation. Frankfurt/M.: Suhrkamp. Engl. (2008): Origins of human communication. Cambridge, MA: MIT Press.
Tonella, G. (2008): Die Funktionen, Bindungen und Interaktionen des SELBST. In: Heinrich-Clauer, V. (Ed.): Handbuch Bioenergetische Analyse. Gießen: Psychosozial-Verlag, 59–111. Engl. (2011): The Self: Its Functions, its Attachments and its Interactions. In: Heinrich-Clauer, V. (Ed.): Handbook Bioenergetic Analysis. Gießen: Psychosozial-Verlag, 57–112.
Trevarthen, C. (2009): The Intersubjective Psychobiology of Human Meaning: Learning of Culture Depends on Interest for Co-Operative Practical Work and Affection for the Joyful Art of Good Company. Psychoanalytic Dialogues, 19, 507–518.
Winnicott, D. W. (1974: Reifungsprozesse und fördernde Umwelt. Frankfurt/M.: Fischer. Engl. (1990): The Maturational Processes and the Facilitating Environment. London: Karnac.
About the Author
Dr. med. Jörg Clauer, born in 1951; CBT and Faculty Member of IIBA. Biochemist, doctor of psychosomatic medicine and psychotherapy- psychoanalysis (DGPT, DPG, IARPP), psychiatry and psychotherapy, general medicine, rehabilitation. For many years, managerial position in psychosomatic specialist clinics, psychotherapeutic practice since 1999. Lecturer, teaching therapist and supervisor (DGSV) in the field psychotherapy, psychoanalysis, bioenergetic analysis, marriage family and life counseling, coaching, organizational consulting. Various publications in books and journals. Founding member of EfBAP, editorial staff member of the Forum Bioenergetic Analysis.
E-mail: joerg.clauer@osnanet.de