Body Resonance and the Voice1
Vita Heinrich-Clauer
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2016 (26), 137–157
https://doi.org/10.30820/0743-4804-2016-26-137 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstracts
English
This article focuses on bioenergetic principles and the link between emotions and the voice, discussing various approaches to vocal expression in the psychotherapeutic process. There is an examination of the idiosyncrasies of bioenergetic work with the voice in contrast to therapeutic approaches that work solely with the body. There is an important distinction for practical bioenergetic work between liberating vocal discharge on the one hand and the build-up of tone, boundaries and self-efficacy on the other hand (cf. Shapiro, 2006, 2008, 2009).
Key words: bioenergetic vocal expression, vocal discharge, charging-containing, tonicity.
German
Dieser Beitrag zielt auf bioenergetische Prinzipien in Bezug auf die Verknüpfung von Emotion und Stimme. Verschiedene Ansätze zum stimmlichen Ausdruck im psychotherapeutischen Prozess werden diskutiert, wobei die Besonderheiten bioenergetischer Arbeit mit der Stimme im Unterschied zu reinen körpertherapeutischen Ansätzen herausgestellt werden. Es gibt eine wichtige Unterscheidung in der praktischen bioenergetischen Arbeit: einerseits kann eine befreiende stimmliche Entladung (discharge) und andererseits eine tonisierende, die Grenzen und Selbstwirksamkeit fördernde Vorgehensweise bewirkt werden (charging-containing, vgl. Shapiro, 2006, 2008, 2009).
French
Cet article met l’accent sur les principes d’analyse bioénergétique et le lien existant entre émotion et voix en analysant diverses approches à l’expression vocale à l’intérieur du processus thérapeutique. On y examine les idiosyncrasies propres au travail d’analyse bioénergétique avec la voix en opposition aux approches thérapeutiques travaillant uniquement avec le corps. Il existe une différence importante en matière de travail pratique en analyse bioénergétique entre la décharge vocale d’une part et le développement du ton, des frontières et de l’efficacité, d’autre part. (cf. Shapiro, 2006, 2008. 2009).
Spanish
Este artículo se centra en los principios bioenergéticos y la relación entre las emociones y la voz, y trata de diversos enfoques acerca de la expresión vocal en el proceso psicoterapéutico. También presenta una evaluación de la idiosincrasia del trabajo bioenergético con la voz, en contraste con los enfoques terapéuticos que se centran únicamente en el cuerpo. Hay un distinción importante para el trabajo bioenergético práctico entre por una parte, liberar la descarga vocal, y la acumulación de tono, límites y la autoeficacia por la otra (cf. Shapiro, 2006, 2008, 2009).
Portuguese
Este artigo focaliza princípios bioenergéticos e a conexão entre as emoções e a voz, discutindo várias abordagens da expressão vocal no processo psicoterapêutico. Avalia, ainda, as idiossincrasias do trabalho bioenergético com a voz, em contraste com abordagens terapêuticas que trabalham somente o corpo. Mostra, também, que há uma importante distinção, para a prática do trabalho bioenergético, entre a liberação de uma descarga vocal, de um lado e a construção do tom, limites e auto-eficácia de outro (cf Shapiro, 2006, 2008, 2009).
1. Introduction
An embodied voice transmits and reveals something about the truth of our own person. The sound of our voice offers a more genuine form of self-expression than our speech, which is controlled by the left hemisphere of our brain. Free vocal expression can help release pent up emotions, animate our bodies and touch the people around us. The resonant voice reflects, even more than the speaking voice, something about our current internal state and our current mood, as well as about deeper levels of our selves (cf. Alavi Kia in, 2001, 2009). The sound of the voice lets us differentiate one emotion from another based on tempo, articulation and pitch, as well as the corresponding length of the intonation of vowels and consonants.
“The voice is so closely linked to your personality that […] a patient’s neurosis can even be diagnosed from a voice analysis” (Lowen, 1979, p. 236).
And:
“A balanced voice consists of a harmonious combination of chest and head tones. An unbalanced voice inevitably points to a personality problem” (ibid., p. 238).
Wilhelm Reich and Alexander Lowen have – in contrast to Sigmund Freud – convincingly taught the essential importance of working with breath and the voice to facilitate opening to deeper emotions and to more vibrant vitality. Reich was the first to discover that physical work with a client’s breath can open up a special gateway to memories and emotions. In doing so, he distanced himself from the abstinent, verbal, psychoanalytic technique of Freud.
Every bioenergetic analyst is familiar with working with the breath, with energy flow and with vocal expression, since it is one of the basic pillars of our method – in addition to work on grounding. Bioenergetic Analysis has taught us to “release the sound.” Lowen primarily speaks of a “liberation” of sound. However, it is not easy to express oneself in a spontaneous way that comes from your true self! The energetic “door opener” that is the voice deserves more attention in bioenergetic therapy. Simply encouraging clients to just let the voice “come” is not enough since frequently it doesn’t come at all. Or it may emerge as a vegetative expression (sometimes referred to as body memory) without reference to a clear feeling and without a relationship context.
Lowen’s first session with Reich: “vegetative screaming from bioenergetic techniques without reference to emotions”
As I was lying on the bed, nothing happened at first. Reich: “Lowen, you’re not breathing at all” (my chest remained motionless while breathing). After some time breathing again while lying down “Reich commanded: ‘Lowen, let your head fall back and open up your eyes wide!’ I did so, and […] had to suddenly scream out loud” (Lowen, 1979, p. 10f.).
“Oddly enough, the scream did not disturb me. I had no emotional relationship to it.” After repeating the procedure: “The scream ‘came’ once again. I don’t want to say that I was screaming because I wasn’t under the impression that I was doing it. The scream just ‘happened’ to me. Once again, I had actually nothing to do with it at all” (ibid., p. 11).
“When the session was over and I had left Reich, I had the feeling that not everything was as alright with me as I had thought. There were ‘things’ – images, emotions – in my personality that were hidden from my conscious mind, and then I realized that they had to come out” (ibid.).
After a year of therapy with Reich: “sobbing triggered by connotative words relating to emotions”
“After a year of therapy, I was at an impasse. Since we saw no way out, Reich suggested I discontinue the therapy. ‘Lowen,’ he said,’ you’re simply unable to give in to your feelings. Don’t you think you should stop?’ His words were a condemnation. Quitting would have meant the end of my dreams. I broke down and cried. It was the first time since childhood that I was sobbing. I could no longer hide my feelings. I told Reich what I wanted from him and he listened attentively. I still do not know whether Reich wanted to actually quit the therapy or whether his proposal was only a maneuver to break my internal barrier. In any case, at the time I was under the impression that he was serious. And the result was that the therapy took effect again” (ibid., p. 14).
“After the crying fit and the expression of my feelings towards Reich, my breathing became lighter and freer, my sexual responsiveness deeper and more complete” (ibid.).
2. Various Approaches to Working with the Voice in Body Oriented Psychotherapy
The focus on the breath and the vocal expression of emotions is an important aspect of many body psychotherapies – unfortunately not of every psychotherapy! There are important differences in working with the voice in bioenergetic analysis and in pure body therapies, as well as between bioenergetics and other emotion centered body psychotherapies. Below is an overview of the most well-known methods with a focus on the voice.
Body therapy (practical-functional)
- Vocal and theatrical training (Kristin Linklater, Alavia Kia)
- Laughter Yoga, bipolar breathwork, respiratory therapy (Ilse Middendorf)
- Martial arts (Wen Do, Karate, Kung Fu, etc.)
Body psychotherapy (biographical, centered on emotion)
- Primal therapy (primal scream, Janov)
- Greek mourning ceremonies (J. Canacakis)
- Other body oriented psychotherapies: Biosynthesis, Core Energetics, Biodynamics, Psychodrama, Gestalt, Analytic Body Psychotherapy, Sensory-motor Psychotherapy
- Bioenergetic Analysis (Lowen, Bob Lewis, Ben Shapiro)
A second glance reveals the fundamental differences in these approaches, particularly from the standpoint of a cognitive-verbal oriented “top-down” vs. energetic-somatic “bottom-up” processes. Furthermore, we see how difficult it is to integrate a kind of “doing the sound” with emotional comprehension and self-regulation. And not many approaches focus on that.
It is important to look at how the client is invited to learn about his/her voice. Do we rely on verbal interventions only or do we trust the body in a more basic sense? We may start by verbally exploring memories regarding the voice or “landscapes of dealing with vocalizations in the family.” It is useful to explore this biographical information within the framework of resistance analysis and not to rush into the bioenergetic mode of “making a sound.” One might ask, “Who was allowed in your family to be loud? When? Where? Were sounds of pain permitted? Or was the message, ‘Boys don’t cry!’”? Were joyful sounds heard in the family?” We can verbally explore in the here and now with the question: “What sound might belong to this sensation or memory?” This is often answered with, “to make sounds and noise is too embarrassing to me, especially on command.” This vocal self-inquiry may initially be met with a considerable shame barrier (cf. Moser, 2013, p. 452f.).
If this therapeutic approach is formulated in the subjunctive – on the left-hemispheric level – clients are asked to reflect on and, at most, produce a sound. We, too, are aware of this response from our clients in bioenergetic therapy. Also, the response often not only reveals the shame the client feels, but also their clear refusal to have to do something that is just not that easy to do.
In bioenergetic analysis we focus on biographical and on relational aspects in the here and now of the therapeutic encounter as well as on energetic processes (catharsis vs. containment). We can rely on a variety of basic bioenergetic interventions to foster vocal expression in order to work with emotional regulation. In chapter 5 and 6 energetically based interventions will be addressed.
3. On the Neurophysiology of the Voice and Relationship: Porges’ Polyvagal Theory
Charles Darwin believed that both language and music emerged from a common musical “proto-language” used to communicate emotions, territorial behavior and during courtship (cf. Darwin, 2000). The voice touches the other and enables communication without words. The resonance of the social environment is solicited via timbre, melody and volume (social overture, seeking an echo). In psychotherapy, the rhythm and amplitude of the therapist’s own breathing is critical in detecting the body and feelings of the client. The difference between pure body therapies, such as massage, physiotherapy, osteopathy, etc. and bioenergetic analysis is found when one understands that in bioenergetic analysis the relationship-creating gestures or bodily contact tied to relationship images stimulates clients reactions via the ventral vagus.
Calming yourself and calming the other person in threatening situations is another special feature of the voice.
Facial Expression and Vocalization
Porges’ Polyvagal Theory (2010) has given us the tripartite structure of the autonomic nervous system (ANS): in addition to the sympathetic fight-flight reaction, the vagus is also divided into a dorsal vagal complex (= DVC) that originates in the dorsal brainstem and a ventral vagal complex (= VVC) that originates in a ventral originating core. The DVC is regarded as a relic of an immobilization system from the reptilian era. During conditions of rest, it stimulates regular digestive processes. Existential threatening situations, however, lead to a massive stimulation of the DVC with immobilizing and death feigning/dissociative reactions (Porges, 2010, p. 165). The VVC facilitates experiencing and expressing primary emotions and social communication. There is a coupling for regulating gaze and attention, facial expressions, prosody and the ability to listen (ibid., p. 75f; cf. also Clauer, 2013, p. 283–285).
The ventral vagus complex (VVC), which comprises the NA (ventral nucleus ambigus) and the nuclei of the trigeminal and facial nerves, is clearly related to expression and the experience of emotions (ibid., p. 77). The capacity for social engagement depends on how well we can influence our facial and cranial muscles using nerve (corticobulbar) pathways that interconnect the cortex and the brain stem. These muscles make our face capable of showing expression and allow us to communicate meaning through gestures, to influence the sound of our voice, to turn our gaze to specific things and to use our hearing to differentiate human voices from background noise. The neuronal control of facial and cranial muscles influences how people perceive the efforts of others to enter into relationship with them.
A negative affective state (negative primary emotion) would reduce the tone of the entire vagal branch (VVC). It originates in the NA geared to promoting fight or flight behavior. A reduced tone (triggered by an external or internal threatening situation) leads to reduced social engagement:
- The eyelids droop.
- The voice loses its ability to modulate, gets flat.
- Positive facial expressions are rare.
- The sound of human voices is perceived indistinctly.
- Sensitivity of the efforts by others to establish social contact decreases.
A higher VVC tone (seen in secure situations) allows one to:
- express oneself with an appealing vocal tone and speech rhythm,
- show a friendly facial expression,
- influence middle ear muscles in such a way that human voices can be clearly distinguished from background noise,
- make eye contact, and
- to have a reduction of social distance (cf. ibid., p. 35f.).
In socially safe situations, the “prosocial” VVC, with its so-called vagal brake, therefore inhibits the mobilizing fight or flight readiness of the sympathetic nervous system and the immobilizing emergency reactions of the DVC. The concept of neuroception describes a person’s vigilant scanning of the environment for hazards and existential threats.
“The neuroception of familiar people as well as people with a confidence-inspiring and empathetic sounding voice and a corresponding facial expression leads to a social interaction that promotes a sense of security” (ibid., p. 90).
Porges provides evidence of hemispheric differences and a vagal lateralization, according to which a relationship exists between the function of the right hemisphere and primary emotions.
“The primary chronotropic output of the heart comes from the right NA (ventral nucleus ambigus) via the right cardiac vagus nerve. The special visceral efferent fibers that allow behaviors through which emotions are defined (facial expression and vocalization) also have a right hemispheric tendency and are neuroanatomically connected to the general visceral efferent fibers emanating from the NA that regulate the bronchial tubes and the heart – organs assumed to be sensitive to emotions and stress” (ibid., p. 76).
These neurophysiological studies do not make a distinction between the sensation of a negative affective state and their expression. In this case, it would be interesting to see whether differences could be observed in a person’s physiological responses at the ANS level, when there is a way to express emotions such as anger, sadness and joy.
Case Vignette 1
Manual interventions in a situation where one has no opportunity to make a sound that reflects pain and is in an insecure therapeutic relationship
A currently clearly depressed client reports her dentist’s intensive work on resetting her jaw. It was enormously strenuous for her to keep her mouth open for the time required, since she has a history of abuse, a long-standing anxiety disorder and social phobia. Because of the massive neck and jaw tension that resulted from her dental treatment, the dentist suggested that she see a physiotherapist for chiropractic and manual therapy. The client says that the well-intentioned physiotherapist’s manual manipulation was even worse than her dental treatment, since she experienced tremendous pain and could not express it. She says that her relationship with her dentist was good but that of her physical therapist lacked warmth and was technically oriented, as he showed no personal feedback whatsoever.
After her session with me she told her physiotherapist at her next appointment that her psychotherapist had told her that moaning or crying in pain would reduce the pain. The physical therapist subsequently closed the windows and was personally attentive to her for the first time. That helped her to have a reduction of pain during the following treatment.
This regulation of the relationship can be understood both in the sense of Porges’ SES and in a bio-energetic sense. The difference between body therapies like massage, physiotherapy, etc. and in bioenergetic analysis (and other body psychotherapies that work with relationships) is that relationship-creating gestures or bodily contact associated with relational images stimulates other reactions via the vagus than the mere mechanical contact of a stranger (cf. section 3).
4. General Bioenergetic Aspects: Movement – Grounding – Breathing – Emotionality – Motility – Stress – Vocal Expression
Our breathing is organized by reflexes. It is a pulsation: contraction – expansion. The breath wave normally flows from our mouth to the genitals.
As long as we breathe, we live. We cannot commit suicide simply by holding our breath. As long as we breathe, we feel. Deep breathing improves the motility of our muscles as well as improving the natural vibration of our body, which is the prerequisite for vocal expression. We can inhale “to the fullest” or restrict our breathing and our vital contact with the environment by placing it (breathing) on the “back burner.” Breathing fully brings pleasure and joie de vivre (although excess oxygen creates an increased drive and a sense of urgency or anxiety). Shallow breathing results in lack of oxygen and limits our vitality and emotion in such a way that we produce little vibrant impulse and correspondingly receive little feedback (classic depressive pattern). The emotional expression while making sounds provides us with stimulation via vibration and self-massage, while reducing rigidity, stiffness, silence, depression and introjects.
Breathing is the central key to perceiving emotions and expressing these with the voice – or to controlling emotions by holding our breath and taking shallow breaths.
Core feelings such as sadness, anger, fear, disgust, desire and joy are kept in check by regulating breathing. “When an emotion is blocked it cannot be expressed well vocally” (Lowen, 1979, p. 237).
The blockage involves all the contractile muscles of the upper body (mouth and jaw muscles, tongue, neck, intercostal muscles, etc.) as well as the pelvic muscles.
The respiratory muscles: diaphragm, intercostal muscles, pelvic floor muscles, shoulder girdle and neck also contract when breathing is restricted.
There is less expansion in the diaphragm between the lowest lumbar vertebrae, the sternum and the lower rib cage.
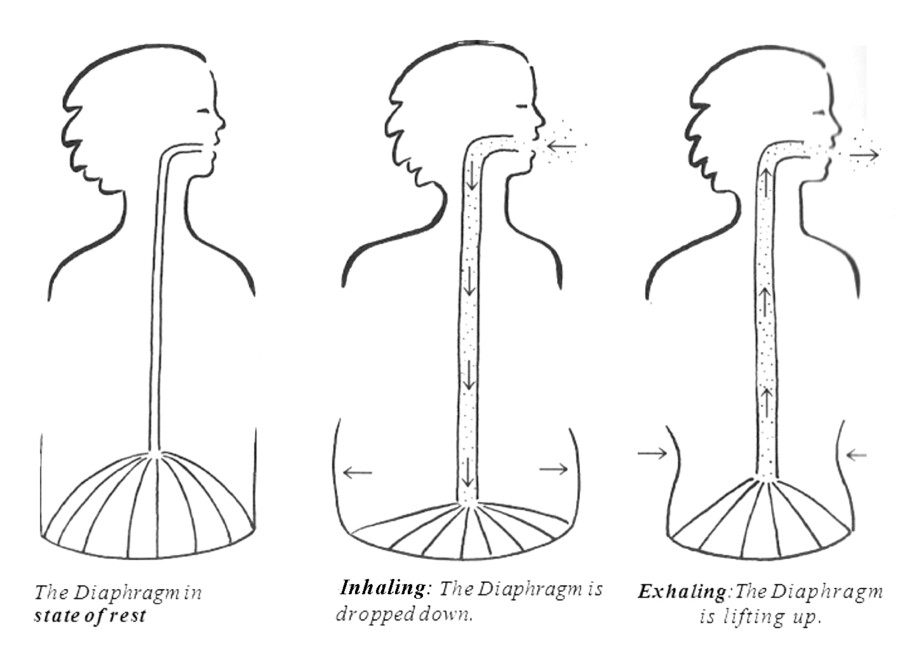
Figure 1. Diaphragmatic movement while breathing
When inhaling, the diaphragm actively moves downward, which creates a vacuum that is followed by the passive inhalation of air through the airways.
Inhalation actively sucks in air and takes in oxygen, which enriches the blood. This offers an intensive “internal contact” with the environment via the surface of the respiratory organs. On the muscular level, the following occurs:
- the diaphragm drops and expands the chest area downwards,
- the ribs open up like blinds,
- the lumbar spine becomes erect (slight hollow back),
- the pelvis pulls itself slightly back,
- the spine makes a wave motion,
- the upper body expands,
- the changed muscle tone and the erect position show tonicity.
Inhalation and the tension in the diaphragm massage the abdominal organs (rhythm of the intestine, bladder, sexual organs, sexuality!). Deep breathing involves all the stabilizing core muscles, including the pelvic floor (grounding and sexuality!).
Exhalation releases air to the environment again (with the waste product carbon dioxide). Discharging air is a relief and a “burden” on the environment. On the muscular level, the following occurs:
- the diaphragm lifts,
- the intercostal and stomach muscles contract,
- the pelvis tilts forward and down,
- the lumbar spine expands backwards and down,
- the upper body loses volume,
- the decreased muscle tone indicates flexibility (possibly emptiness).
When exhaling, the diaphragm moves back up to the fifth/sixth rib, the chest expands, the intercostal muscles stretch. In doing so, the heart is also massaged on the exhalation (sighing, toning, lamenting, liberation from old pain and alleviation of the heart).
Breathing is done by the muscles in the shoulder girdle and neck, which lift the clavicles (opening the esophagus: anxiety crying, sucking in air, taking for yourself).
The following poem by Erich Fried touchingly describes the relationship between exhalation and emotionality:
Revocation
Being able to exhale your unhappiness
Exhale deeply
so that you can inhale again
And maybe being able to articulate your unhappiness
in words
in real words
that are coherent and make sense
that you can still understand yourself
and that perhaps even someone else understands too
or could understand
And being able to cry
That would almost be happiness again
Lowen speaks about “freeing the path of communication from the heart to the world” when we work with segments in the body. There are three segments of the body that can develop rings of tension from chronic holding, which narrow the channel and prevent the full expression of feelings. These tension rings are not anatomical but functional units.
- The outermost segment ring forms around the mouth. A firm or closed mouth can block any communication of feelings. Compressed lips and a locked jaw prevent sounds from making their way out into the open (Lowen, 1979, p. 241).
-
The second segment ring of tension is formed at the junction of the head and neck. It represents the transition from voluntary to involuntary control. The throat and mouth lie in front of this area; the esophagus and trachea are behind it. Things you don’t want to swallow are controlled here. In this segment is an unconscious defense mechanism against the expression of unacceptable feelings. The tension affects breathing and contributes to feelings of anxiety (ibid., p. 241f.).
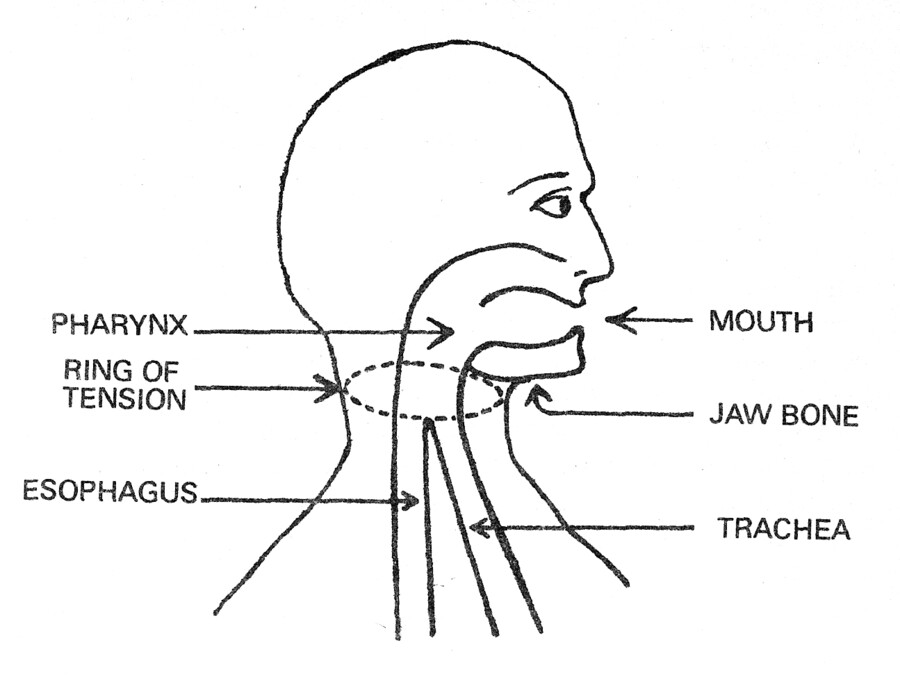
Figure 2. Ring of tension at the junction of the head and neck
- The third segment ring is seen in the connection of the neck and thorax: the front, middle and rear scalene (rib holding) muscles are involved. This ring of tension guards the opening of the rib cage and thus the heart. When these muscles are chronically contracted, they arch up and make the upper ribs immobile which constricts the opening to the chest. Because this obstructs natural respiratory movements, voice production is impaired. This applies particularly to the chest register (ibid., p. 244f.).
According to Lowen, a lack of vibrations indicates stress and holding back either in the body or in the voice.
“A person who does not vibrate is under stress or holding back when it comes to his/her body and his/her voice. In the voice, a lack of vibration leads to a loss of resonance” (ibid., p. 237).
Stress = Holding back = Loss of Vibration = Flatness/Lack of emotions and feelings.
Moreover, shallow breathing, lack of vibration and reduced motility weaken our immune system, while deep breathing, vocal expression, laughter and singing positively stimulate our immune system on the hormonal level. In some clinics, especially in pediatrics, doctors specifically employ “laughter therapy” (e. g. with hospital clowns) in order to take away patients fear of surgery. Laughing patients require fewer painkillers (cf. Spiecker-Henke, 2013; Kreutz, 2014).
In some fifth to sixth grade math classes, screaming is encouraged to promote concentration. According to their math teacher this is enhancing the children’s concentration if it’s done every 20 minutes!
5. Special Features of Bioenergetic Work with Emotions and the Voice: Motoric and Vocal Expression and Hands-on Techniques
Lowen recognizes the need to not only work on emotional blockages but also specifically on the voice in order to loosen tension. In doing so, the focus is more on spontaneous sounds and on the liberation of repressed emotions, via the release of tension in the muscles involved.
The following techniques are used to coordinate motoric and vocal expression:
- Lying down, kicking on a mattress with your legs, while shouting “Why?”, “No!” or “Leave me alone!”
- Hitting foam cubes with a tennis racket, shouting “Hah” or “No”.
- Using a breathing stool, or Pezzi ball to alleviate the pain and sadness of the heart with an “Ah” sound in an elongated exhalation.
Lowen describes various hands-on techniques to open up vocal blockages and release repressed emotions (Lowen, 1979, p. 240f.):
- Putting continuous pressure (a John Pierrakos technique) on the scalene muscles and the sternocleidomastoid muscle. While doing so, the client is encouraged to emit a constant, high-pitched tone. If no scream comes, says Lowen, he stops pressing and accepts the resistance.
- Pressing on the masseter muscle, while the client is lying down and kicking the bed with a loud protesting sound. The opening of the jaw, which he called the “gate of the personality,” is regarded as the key to all other blocking mechanisms in the body.
“Although you can do a good job inducing screams with this method, it still does not reduce all the tension that has formed around the mouth and throat that inhibits generating tones. When a person’s voice is free, it comes from the heart” (ibid., p. 241).
It is important not to assume that a deliberately produced sound (or even the bioenergetic “disposition” of moaning and screaming) too soon is a release. It may be that it represents a physical release of tension only, which is an important first step (see the explanation and Lowen’s first session with Reich earlier in this article).
“If an expression of feeling confirms the self, then the mind and body must always interact. That’s why crying or even screaming has no therapeutic effect as long as we don’t know why we’re crying and aren’t able to talk about it” (cf. Lowen, 1993, p. 74).
Therapists are encouraged to stay attentive and listen to the sounds that reach us to determine whether or not this sound is associated with a core emotion or an authentic non-verbal statement about the self.
In order to spontaneously develop a sound or a spontaneous tone a client may need:
- bioenergetic techniques
- somatic resonance of the therapist
- verbal support and comprehension
- encouragement to express feelings and sounds
If we are experiencing an emotionality, a somatic resonance – specifically in certain areas of the body – and not just an intense loud noise, then we (as therapists) feel emotionally connected to the client. We work with our clients to find an authentic sound with the contact or by using hands-on techniques on the neck, jaw, or even with cooperation (joint toning with the client). In case of any inhibitions, feelings of being stuck or artificial statements about the self, we try to change the client’s expression by requesting the client repeat their sentence again with a relaxed jaw to amplify this without stress in the throat. We may try vocal accompaniment to facilitate a flowing, harmonious and touchingly spontaneous expression.
6. Differentiation of Bioenergetic Concepts and Methodology when Working with Vocal Expression
Discharging Pain, Fear, Anger – Release – Surrender
The voice can be used to provide relief and release in the therapeutic process.
Release takes place in the exhalation, which can free pent up emotions and release the muscle groups involved. Vocal expression with emotional content (pain, fear, anger) generates vibrations and works via the self-massage from the inside, like a sensory confirmation, a surrender to your own body (cf. Lowen, 1993).
“However, the goal of therapy is not only to liberate the voice, but to coordinate free vocal expression with the corresponding free physical expression through movement” (cf. ibid., p. 138).
Coordinating free vocal expression with free physical expression can be seen as follows:
- The voice sometimes lets me discover my mood (self-perception on the auditory and proprioceptive level) and improve my mood. It can offer self-assurance that I am alive, I breathe, I make sound, I am there. I use it to touch myself and others.
- The voice can help me develop harmony with myself (e. g. sighing and plaintive sounds), loosen rigidity and let go of the abdomen and pelvis, experience the resonance of my own body and experience soft feelings. Or I can give room to my rage, by spitting it out instead of swallowing it, or by screaming. A feeling of relief and joy is often the result.
- The voice and the opening of the throat, (the “pipes”) dissolves pain. This is because pain is reduced with crying, which can relax the muscles).
Case Vignette 2:2 Exhalation and Processing Pain
This case study helps clarify the relationship of breathing, vocalization and processing pain based on an excerpt from the 39th therapy session with a 37-year-old man, Mr. F. The client was suffering from anxiety, panic attacks, insomnia and stomach problems. He showed a preference for sadomasochistic practices.
As I firmly massaged his cranial base muscles, he did not utter a sound. After I paused and jokingly told him I don’t intend to break my thumb in today’s session, he replied: “That’s just it! If I don’t make a sound, that increases the pain and the pleasure!”
This statement made a lot of sense, since the client said he was into S&M techniques! I replied, “Oh Gosh, I totally forgot about that.” I was naive, or put positively, I was uninformed regarding S&M techniques. But then I explained that toning and release of (old) pain and anxiety was, among other things, a therapeutic goal of bioenergetic analysis and that all body cells can expand and relax when exhaling. Pain can be reduced when we make a sound.
The client listened attentively to this and said, “Ok, I’ll try to make a sound.”
I told him that his sexual practices/preferences might change when he changes his emotional (pain) processing mode.
He then replied: “Yes, if it happens as you say, I’ll just accept it as such. I’ll take that chance.”
That was what happened: Mr. F. separated from his wife (his S&M companion), fell in love with a less obsessive young woman, switched to “normal” sexual positions and had a child. In addition, he lost his phobia of highway driving and his hypochondriacal fear of a heart attack.
Case Vignette 3: Rage and Fear
A colleague in training discussed her insomnia in an encounter group. Afraid of her first consulting sessions, she was not able to sleep for two nights and was plagued by doubts about her skills. She was not able to sleep in the seminar house. A first diagnosis of her posture while standing revealed raised, tense shoulders and an anxious expression in her eyes. She reported having “frozen shoulder” syndrome. The body-oriented constellation of her relevant biographical scenario revealed the image of her three older brothers who she experienced as a burden on her shoulders and pressed her down. In the past, they would frighten her with their pranks and torture her. She remembers how she had, when she was four years old, once crossed the courtyard in the dark of night to go the outhouse and how her brothers turned off the light as she sat there alone.
She screamed in terror. Her parents did not notice their wicked game in the outhouse or her distress. Today, as an adult, she is not able to scream and feels imprisoned in her body whenever she is confronted by excessive demands. While working on this scenario, she gradually summed up enough courage to raise her voice and shout “Stop it” at a gradually increased pitch until finally emitting a spectacular cry that filled the entire room! As a result, her shoulder muscles relaxed; her frightened eyes relaxed as well. She slept well in the seminar house that night.
At home, she now regularly practices screaming in her car on the way to her counseling work and reports that she is able to sleep again.
Special Exercises that Relax the Voice and Prepare for “Discharge”
Anger/Protest:
Lying on the bed rhythmically kicking and/or crying “Why?” (sound sustained as long as possible). The “Why?” is raised to a scream while quickly and intensely kicking. Shouting while car driving (cf. Lowen, 1993, p. 138).
Jaw/Tongue:
Yawning, making grimaces with the jaw and lips, sticking the tongue out left and right, panting like a thirsty little dog.
Eyes/Head/Neck:
Rolling the head on the floor, receiving a neck massage and toning.
Laughing:
Arching the head backwards, laughing “Ha, ha, ha …” (cf. Shapiro, 2008, p. 79).
Fear:
Imagining something on the ceiling that triggers fear. Then inhaling with the sounds of fear, exaggerate this sound, then lower the head, exhale, and let go (while standing). Next, do the same exercise as the Cow/Cat position in Yoga. (get on the floor, on hands and knees, alternating concave and convex rounding of the back).
Craziness:
Sticking the tongue out to the left and right, make silly laughter, “Meeting of village idiots” (ibid., p. 69).
Sounds fall out:
Lying down, lift the pelvis and drop it to the floor and let a sound fall out while exhaling; in the same position, lift your chest off the ground and drop it to the floor with your upper back, letting a sound fall out while exhaling.
Charging, Toning, Building Boundaries and Containment, Self-Efficacy
Bioenergetic analysis understands resilience and vocal expressiveness as a physical concept. These depend not only on the perception of one’s muscular strength but substantially on the capacity to breathe deeply and to have vocal expression (cf. Heinrich-Clauer, 2014; also Spiecker-Henke, 2013; Kreutz, 2014). The voice may be used to tonify and establish boundaries, that is, to invigorate in the sense of resilience and expressiveness. In this regard, the work of Ben Shapiro in particular represent a complement to and creative extension of the basic bioenergetic techniques since these direct one’s focus on charging, containing and boundary techniques (cf. Shapiro, 2006, 2008, 2009).
Deep inhalation expands the upper body and straightens the thoracic spine. The pelvis pulls back slightly. This allows one to define his/her personal space in relation to the other and to have a contact boundary. The emphasized short inhalation creates the moment of tension! The altered muscle tone and the erect posture demonstrate vigor.
If one takes advantage of this charge to make an increasingly powerfully held sound, instead of letting go when exhaling (as in sighing or moaning), the defining effect is reinforced and this is a charge in the body at the same time (toning).
- Toning is used to strengthen the body’s boundaries, to build up structure and delineate it from the social environment. This allows one to distinguish between me and you.
- Increased self-efficacy through controlled tones: by making oneself noticeable through held and controlled breath, one also appears self-effective in relation to the social world.
Special Exercises to Build up Boundaries and for Containment (Charge)
Boundary, voice:
Partner exercises: standing across from one another, saying: “No – Yes”; “I have the final say!”; “Do it the way I want!”
Boundary, mouth/lips:
Making sharp loud sounds like, “ssssh,” and “pphaa!”
Boundary, diaphragm:
Crying “Hah!” while standing across from a partner, keeping the partner away with forcefully emitted sounds.
Boundary, neck:
Start in the hanging over position against the wall or against the hip of a partner. While pressure is exerted by the upper back, shoulder girdle and neck exhale, raise your voice, making it louder – up to the climax of control! (Don’t wait until the sound decreases.)
Boundary, arms:
Wringing a towel or flex rod, holding your voice as long as you can and maintain the tension in your hands/arms (cf. Shapiro, 2006, p. 161).
Boundary, pelvis:
Taking the semi-position on the breathing stool, moving the jaw out, pushing the pelvis forward while exhaling (or: therapist exerts counter-pressure with her hands).
Containment:
Lying on your stomach, tensing all back and leg muscles, lifting your head, raise your voice, scream “I caaaaaannnn!” – stopping at the peak of your voice/muscle control.
7. Conclusion
The energetic “door opener” that is the voice deserves more attention in bioenergetic therapy. We can rely on a variety of basic bioenergetic interventions to foster vocal expression in order to work with emotional regulation. The emotional expression while making sounds provides us with stimulation via vibration and self-massage while reducing rigidity, stiffness, silence, depression and introjects. But simply encouraging clients to just let the voice “come” is not enough since frequently it doesn’t come at all. It is important not to assume that a deliberately produced sound (or even the bioenergetic “disposition” of moaning and screaming) too soon is a release. There is an important distinction for practical bioenergetic work between liberating vocal discharge on the one hand and the build-up of tone, boundaries and self-efficacy on the other hand. The voice may be used to tonify and establish boundaries, that is, to invigorate in the sense of resilience and expressiveness.
From a bioenergetic point of view, it is worthwhile to note the expressive gestures of celebratory athletes on the sports pages of your newspaper. Cf. Video (YouTube): All Blacks Haka. It will become unfortunately clear that our profession hardly provides this kind of an opportunity to open your mouth and raise your fist in victory. A pity, really!
Footnotes
- [1]
- Lecture delivered March 7th, 2014 in Papenburg, Germany at NIBA’s student information day.
- [2]
- This case has been described in more detail in another therapy sequence published by Clauer and Heinrich 1999. For this publication, the client’s consent was given so that the current description of the case does not breach the rules of patient confidentiality.
References
Alavi Kia, R.(2001). Stimme – Spiegel meines Selbst. Bielefeld: Aurum Publishers.
Alavi Kia, R.(2009). Die Musik des Körpers. Integratives Stimmtraining. Bielefeld: Aurum Publishers.
Clauer J. & Heinrich, V. (1999). Körperpsychotherapeutische Ansätze in der Behandlung traumatisierter Patienten. Psychother. Forum, 7, p. 75–93.
Clauer, J. (2013). Psychovegetative Regulation, Kooperation, Triade und das Grounding-Konzept der Bioenergetischen Analyse. In M. Thielen (ed.), Körper – Gruppe – Gesellschaft (p. 277–286). Gießen: Psychosozial- Publishers.
Darwin, C. (2000). Der Ausdruck der Gemütsbewegungen bei dem Menschen und den Tieren. Frankfurt/M.: Eichborn Publishers.
Heinrich, V. (1997). Körperliche Phänomene der Gegenübertragung. Therapeuten als Resonanzkörper. Forum Bioenergetische Analyse, p. 32–41.
Heinrich-Clauer, V. (ed.). (2008). Handbuch Bioenergetische Analyse. Gießen: Psychosozial Publishers.
Heinrich-Clauer, V. (2009). Die Rolle der Therapeutin in der Bioenergetischen Analyse. Resonanz, Kooperation, Begreifen. In P. Geißler & V. Heinrich-Clauer (ed.), Psychoanalyse & Körper, Nr. 15 [Sonderheft: Bioenergetische Analyse im Dialog], 8, p. 31–55.
Heinrich-Clauer, V. (2013). Wirkfaktoren der Gruppe aus Sicht der Bioenergetischen Analyse. In M. Thielen (ed.), Körper – Gruppe – Gesellschaft (p. 111–121). Gießen: Psychosozial Publishers.
Heinrich-Clauer, V. (2014). Bioenergetische Selbstfürsorge für Therapeuten – Zwischen Öffnung und Abgrenzung. Forum Bioenergetische Analyse 2014, p. 9–33.
Kreutz, G. (2014). Warum Singen glücklich macht. Gießen: Psychosozial Publishers.
Linklater, K. (1976). Freeing the Natural Voice. New York: Drama Publishers. Dt. (2001): Die persönliche Stimme entwickeln. Ein ganzheitliches Übungsprogramm zur Befreiung der Stimme (2nd edition). Munich: Ernst Reinhard.
Lowen, A. (1979). Bioenergetik. Therapie der Seele durch Arbeit mit dem Körper. Reinbek: Rowohlt Publishers.
Lowen, A. (1993). Freude. Die Hingabe an den Körper und das Leben. Munich: Kösel.
Moser, T. (2013). Auf der Suche nach dem stimmigen Ton. Deutsches Ärzteblatt PP, 12(10), p. 452–453.
Porges, St. (2010). Die Polyvagal-Theorie. Neurophysiologische Grundlagen der Therapie. Emotionen, Bindung, Kommunikation und ihre Entstehung. Paderborn: Junfermann.
Shapiro, B. (2000). Will Iceberg Sink Titanic? Bioenergetic Analysis, 11(1), p. 33–42.
Shapiro, B. (2006). Bioenergetic Boundary Building. Bioenergetic Analysis, 16, p. 153–178.
Shapiro, B. (2008). Your Core Energy is Within Your Grasp. Bioenergetic Analysis, 18, p. 65–91.
Shapiro, B. (2009). Rekindling Pleasure: Seven Exercises for Opening your Heart, Reaching Out and Touching Gently. Bioenergetic Analysis, 19, p. 53–84.
Spiecker-Henke, M. (2013). Leitlinien der Stimmtherapie. Stuttgart: Thieme Publishers.
About the Author
Dr. Vita Heinrich-Clauer, Dipl. Psych., former researcher and teacher at the University of Osnabrück in psychological diagnostics, psychosomatic medicine, physical diagnostics, and developmental psychology. Since 1989, psychotherapist in private practice, supervisor, lecturer, writer, international trainer for bioenergetic analysis (IIBA faculty).
E-mail: vita.heinrich-clauer@osnanet.de