Searching for Active Factors in Diverse Approaches to Psychotherapy – Types of Intervention and Temporal Aspects
Brief Research Report1
Margit Koemeda-Lutz, Aureliano Crameri, Peter Schulthess, Agnes von Wyl & Volker Tschuschke
Bioenergetic Analysis • The Clinical Journal of the IIBA, 2016 (26), 119–136
https://doi.org/10.30820/0743-4804-2016-26-119 CC BY-NC-ND 4.0 www.bioenergetic-analysis.comAbstracts
English
This paper is a synopsis of scientific research on treatment effectiveness of ten varying approaches to psychotherapy. Different types of psychotherapy justify their existence by the basic assumption that therapeutic change is effectuated by specific concepts, attitudes and interventional techniques. In comparative psychotherapy research, for many years, studies have quantified outcome differences (see e. g. Lambert, 2013), and only very few have closely examined the process of treatment. The study reported here was part of a larger multi-center naturalistic process-outcome study (pre-post-follow-up, see e. g. von Wyl et al., 2013; Crameri et al., 2015; Tschuschke et al., 2015), named PAP-S, which included 362 patients from 81 therapists. The synopsis includes methods as well as results and discussion.
Key words: naturalistic process outcome study, treatment effectiveness research, synopsis, psychotherapy approaches
German
Im Rahmen einer Studie zur Wirksamkeit von zehn unterschiedlichen Therapiemethoden berichtet dieser Beitrag über eine vergleichende Untersuchung von verbalem Therapeutenverhalten in konkreten Sitzungen. Unterschiedliche Therapiemethoden rechtfertigen ihre Existenz mit der Grundannahme, dass therapeutische Veränderung durch spezifische Konzepte, Haltungen und Interventionstechniken bewirkt werde. In der vergleichenden Psychotherapieforschung wurden über Jahre Ergebnisunterschiede quantifiziert, nur sehr wenige Studien haben den Behandlungsprozess näher untersucht. Die hier berichteten Ergebnisse basieren auf Daten aus einer naturalistischen, multizentrischen Prozess-Ergebnisuntersuchung (prä, post und katamnestisch), PAP-S, die 362 Patient/innen von 81 Therapeut/innen einschloss. Der Beitrag beschreibt die verwendeten Methoden, berichtet Ergebnisse und diskutiert sie.
French
Faisant partie d’une étude plus large portant sur l’efficacité de dix approches différentes à la psychothérapie, cet article fait état d’une recherche comparative s’intéressant au comportement à l’intérieur d’une séance. Différents types de psychothérapies justifient leur existence en tenant pour acquis que le changement au plan thérapeutique s’explique à partir de concepts, d’attitudes et de techniques d’intervention. Dans de domaine de la recherche comparative en psychothérapie, et ce pendant plusieurs années, les études ont cherché à quantifier les différences en termes de résultats et très peu d’entre elles ont examiné de près le processus de traitement en soi. Les résultats dont il est fait mention ici se fondent sur des données provenant d’une étude multi-centre sur l’impact du processus, menée dans le contexte d’un environnement naturel (en angl. a multi-center naturalistic process-outcome study) (pré-post follow-up), appelée PAP-S. Elle inclut 362 patients suivis par 81 thérapeutes. L’article présente la méthodologie utilisée, les résultats ainsi qu’une discussion de ceux-ci.
Spanish
Como parte de un estudio más amplio sobre la eficacia de los diez enfoques diferentes en la psicoterapia, este ensayo informa sobre una investigación comparativa del comportamiento en la sesión terapéutica. Diferentes tipos de psicoterapia justifican su existencia basado en el supuesto de que el cambio terapéutico se efectúa por determinados conceptos, actitudes y técnicas de intervención. Durante muchos años, en la investigación comparativa de la psicoterapia los estudios han cuantificado las diferencias de resultado y sólo muy pocos han examinado muy de cerca el proceso del tratamiento. Los resultados que aquí se reportan se basan en los datos de un estudio de proceso-resultado multicentro naturalista (pre-post-seguimiento), llamados PAP-S, en el que participaron 362 pacientes de 81 terapeutas. El documento incluye métodos, así como resultados y discusiones.
Portuguese
Sendo parte de um estudo mais amplo sobre a efetividade de dez abordagens diferentes de psicoterapia, este artigo relata uma investigação comparativa do comportamento terapêutico dentro de uma sessão. Diferentes tipos de psicoterapia baseiam sua existência na suposição básica de que a transformação terapêutica ocorre através de conceitos, atitudes e técnicas de intervenção específicos. Durante um longo tempo, estudos de pesquisa comparativa de psicoterapias têm apontado diferenças quantitativas nos resultados, mas somente muito poucas têm examinado, mais atentamente, o processo de tratamento. Os resultados aqui relatados se baseiam em dados originados num processo naturalista multicentrado de um estudo de resultados (follow up pré e pós), denominado PAP-S, do qual participaram 362 pacientes de 81 terapeutas. O artigo inclui métodos, resultados e discussão.
1. Introduction
Interventional behaviour of psychotherapists is usually based on theoretical concepts from specific psychotherapeutic approaches and technical recommendations derived thereof. They imply anthropological assumptions, premises about health and health disorders, as well as theories of change.
Different types of psychotherapy justify their existence by the basic assumption that therapeutic change is effectuated by specific concepts, attitudes and interventional techniques. In comparative psychotherapy research, for many years, studies have quantified outcome differences (see e. g. Lambert, 2013), and only very few have closely examined the process of treatment. The majority of research so far has failed to prove that approaches under examination actually implemented techniques which they claim to be specific to their type of psychotherapy (see e. g. Perepletchikova et al., 2007).
The study which is reported here was part of a larger multi-center naturalistic process-outcome study (pre-post-follow-up, see e. g. von Wyl et al., 2013; Crameri et al., 2015; Tschuschke et al., 2015), named PAP-S, which included 362 patients from 81 therapists and ten different types of psychotherapy. Patients were from a wide and heterogeneous diagnostic range. Diagnoses (SKID (First et al., 2012), OPD (2001), Global Assessment Functioning Scale (APA, 1989), and Axes I, II, and V, DSM-IV (APA, 1994) were assessed by external experts.
| Type of psychotherapy | Participating institutes | Founders | Main approach |
| Analytical Psychology | C. G. Jung Institute, ISAP, SGAP | C. G. Jung | Psychodynamic |
| Art and Expression Oriented Therapy | Europäische Gesellschaft für Interdisziplinäre Studien (EGIS) | P. J. Knill | Integrative |
| Bioenergetic Analysis | Schweiz.Gesellschaft für Bioenergetische Analyse und Therapie (SGBAT, DÖK) | A. Lowen | Body oriented, psychodynamic |
| Existential Analysis and Logotherapy | Institut für Logotherapie und Existenzanalyse (ILE, GES) | V. E. Frankl | Humanistic |
| Gestalt Therapy | Schweizerischer Verein für Gestalttherapie (SVG) | F. Perls | Humanistic |
| Integrative Body Psychotherapy | Integrative Body Psychotherapy (IBP) | J. L. Rosenberg | Body oriented, integrative |
| Process Oriented Psychotherapy | Institut für Prozessarbeit (IPA) | A. Mindell | Psychodynamic |
| Psychoanalysis (PSZ) | Psychoanalytisches Seminar Zürich (PSZ) | S. Freud | Psychodynamic |
| Transactional Analysis | Schweizerische Gesellschaft für Transaktionsanalyse (SGTA, ASAT) | E. Berne | Humanistic |
Table 1. Types of Psychotherapy Investigated
In the present study we investigated therapists’ interventional behaviour, who claimed to be affiliated with one of eight different types of psychotherapy: Psychoanalysis (Freud, 1895–1940), Art and Expression Oriented Psychotherapy (Knill et al., 1995), Bioenergetic Analysis (Lowen, 1958), Existential Analysis and Logotherapy (Frankl, 1956–1999), Gestalt Therapy (Perls et al., 1951), Integrative Body Psychotherapy (Rosenberg et al., 1996), Process Oriented Psychotherapy (Mindell, 1998), and Transactional Analysis (Berne, 1961).
Our aims were twofold: First, to assess how frequently therapists actually employed interventions specific to their own approach under naturalistic conditions, versus how frequently they employed interventions specific to other approaches or interventions that were common across all approaches. Would therapists’ affiliation with a certain type of psychotherapy predict their interventional behaviour? In case it didn’t, which other factors would? Secondly, we headed for identifying types of intervention used by therapists that systematically engendered lengthy (> 120 seconds) interaction units between therapist and patient. If such types of intervention existed, we hypothesized, they might involve more complex and “deeper” levels of processing in patients, possibly indicating processes of change. Unfortunately, we found only very few other studies investigating temporal aspects of therapist-patient interactions (Duncan, 1972; Rochet-Caplan & Fuchs, 2014; Langs & Badalamenti, 1990; Badalamenti & Langs, 1991).
2. Method
The data presented here are based on two studies (Koemeda-Lutz et al., 2016 a in print; 2016 b, in print). This report focusses on the second one.
2.1. Sample
Out of a total of 13’351 sessions, audio-recorded between 2007 and 2013, a sample of 422 sessions from 92 patients and 42 therapists was drawn. Patients were comparable to other outcome studies, concerning diagnoses, sex and age, as well as socioeconomic data (von Wyl et al., 2013).
As to be expected in a naturalistic study we fell short of reaching an ideal distribution of variables: ideal would have been an equal number of therapists representing each type of psychotherapy, 3 patients from each therapist, and 3 sessions per patient, one from the beginning, one from the middle and one from the end of therapy.

Table 2. Sample
Table 2 shows the actual distribution falling short of our stratification goals – due to patient and therapist drop-outs, recordings of poor acoustic quality etc.
2.2. Variables
Therapeutic interventions were coded according to a rating manual (PAP-S-RM, Tschuschke et al., 2014) by 5 raters, students of psychology, who were not trained in any type of psychotherapy and who were blind with respect to therapists’ affiliations as well as to the attribution of types of intervention to types of psychotherapy. Table 3 gives an example of one such intervention category Focus on emotional experiencing.
| Category 8: Focus on emotional experiencing |
| Definition |
| Therapist’s questions aim at exploring patient’s quality of experiencing, sensations, and feelings. Beliefs, appraisals, explanations or assumptions are not areas of inquiry. Therapist guides patient to focus on her/his present experiencing, sensations, and feelings (to which the patient supposedly has conscious access). |
| Operationalization |
| Therapist |
| – asks about present state of being |
| – asks about present quality of experiencing |
| – clarifies on an emotional level |
| Differentiation |
| ↔ (19) shifting focus of attention to present emotion, of which the patient supposedly is unconscious |
| ↔ (55) clarifying inquiry: exploration of facts, events, cognitions, not emotions |
| Examples |
| 1) How do you experience this? How do you feel about it? |
| 2) You explained to me the way this happened and why Mr. F. did what he did, but I would like to know how you feel about it. |
Table 3. Intervention Category from Rating Manual (Tschuschke et al., 2014)
For each therapist speech turn, coders assigned one of 100 interventions identified in the Rating Manual as a common intervention, an approach-specific intervention, or a specific intervention from other approaches.
| Psychoanalysis (PSZ) |
| 1. Confronting defenses |
| 11. Working on preconscious material |
| 15. Encouraging free associations |
| 27. Interpretation ( SGBAT) |
| 29. Working through painful insights, irretrievable losses, etc. |
| 40. Countertransference (C.G. Jung, BAT ) |
| 55. Clarifying inquiry / exploration (C, GES ) |
| 60. Confrontation |
| 90. Discussing transference (C.G. Jung, BAT) |
| Bioenergetic Analysis (SGBAT, DÖK) |
| 2. Affect regulation (SVG) |
| 17. Breath work (IBP) |
| 27. Interpretation (PSA) |
| 35. Experimenting with novel behavior (SVG, TA, CBT) |
| 40. Countertransference (C.G. Jung, PSA) |
| 56. Promoting somatic experiencing SVG, IBP) |
| 57. Focusing on physical impulses (SVG, IBP) |
| 58. Teaching a body exercise |
| 61. Congruence, sensing incongruence (SVG, Rogerian) |
Table 4. Approach Specific Interventions (approaches also claiming them as specific in brackets)
Table 4 presents intervention categories which proponents from Psychoanalysis and from Bioenergetic Analysis, respectively, claimed to be specific to their approach. As can be seen, some categories were claimed by both types of psychotherapy as specific to their approach (specific but not unique): transference, countertransference and interpretation.
The interrater reliability on a single intervention basis was assessed for 80 sessions. Interventions were coded independently by two students. This resulted in a Kappa coefficient of 0.68 (Cohen, 1988), which according to Landis and Koch (1977, p. 165) can be qualified as “substantial strength of agreement.”
For the investigation of temporal aspects the onset of therapists’ utterances, consisting of at least one complete sentence was recorded. Therapists’ utterances in the investigated sample of 422 sessions amounted to a total of N = 18’542 interventions. The duration of intervals from the onset of one intervention to the next was computed (= 1 interaction unit). For simplicity’s sake therapists’ utterances were called “interventions” and patients’ utterances “reactions.” From a systemic point of view this could, of course, be reversed.
3. Results
3.1. Categorial Aspects: Descriptive
External raters identified on average 43 interventions and 15 different types of intervention per session. Only 14% of all interventions were specific to therapists’ own type of psychotherapy. 66% were common and 20% were interventions specific to other types of psychotherapy. The number of interventions (8 to 173) and their specificity (0 to 57% and 2 to 78%) varied considerably from session to session. A little more than one third of all interventions were specific (34%), 1.4 times as many from other approaches than from therapists’ own. Figure 1 reveals that Process-Oriented Psychotherapists used least and Psychoanalytic Therapists the most specific interventions. This result will be commented on in the discussion.
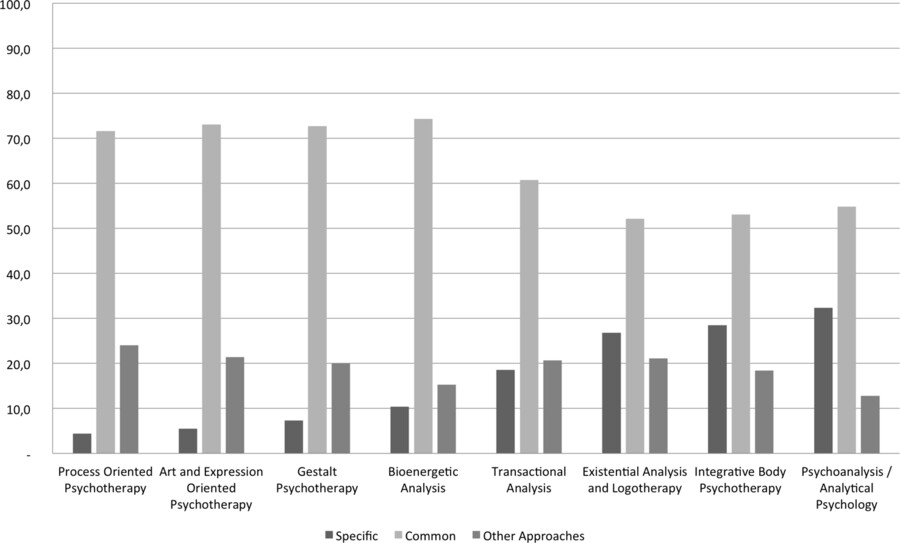
Figure 1. Types of intervention, mean frequences (%)
In all types of psychotherapy investigated, three categories of intervention played a dominant role. They were clarifying inquiry, advice/information, and support (in total 37%, see table 5, left column). All three are common categories, shared by a variety of types of psychotherapy. The total number of common, approach-specific, and specific to other approaches interventions across all of the sessions were tallied and a one-way ANOVA was conducted to determine if therapists’ use of common and approach-specific interventions differed according to their self-identified approach. Results showed that therapists’ professed adherence notwithstanding, the majority of interventions used were common to all approaches, while the interventions used least were those specific to therapists’ self-identified approach (see figure 1).
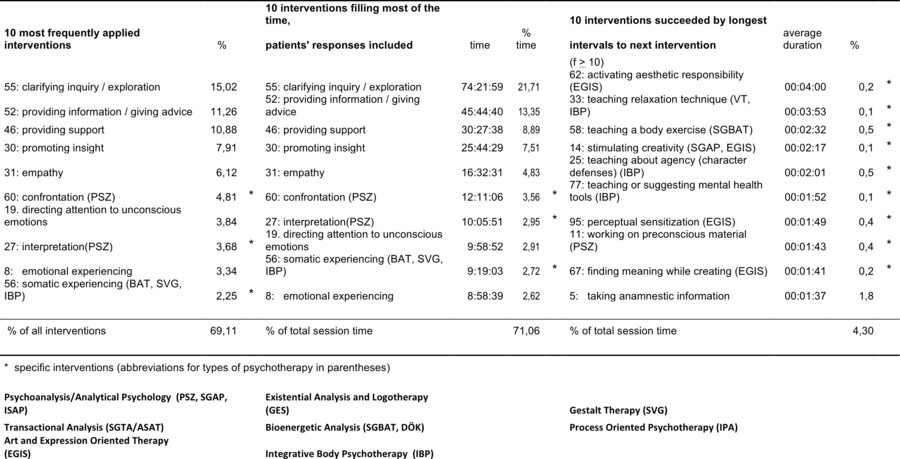
Table 5. The 10 Most Frequently Applied, the 10 Most Time Consuming, and the 10 Types of Interventions Followed by Intervals of On-Average Longest Duration (N = 422 sessions)
3.2. Categorial Aspects: Predictive
Multilevel Modelling
To answer the question of which factors predict the use of different types of intervention,
| No. | Intervention category | Error probabilities and levels of significance | |||||
| approach | p | therapist | p | patient | p | ||
| 1 | Confronting defenses (PSA) | 1,0000 | 0,6575 | 0,0207 | * | ||
| 5 | Taking history information (C) | 0,9998 | 0,9994 | 0,0000 | *** | ||
| 8 | Emotional experiencing (C) | 0,9993 | 0,1470 | 0,0003 | *** | ||
| 11 | Working on preconscious material (PSA) | 1,0000 | 0,9999 | 0,0000 | *** | ||
| 12 | Using humor (C) | 0,9999 | 0,0003 | 0,0000 | *** | ||
| 19 | Directing attention to unconscious emotions (C, SVG) | 0,9999 | 0,0226 | * | 0,0000 | *** | |
| 21 | Exploration of behavioral patterns and beliefs (C, SVG, TA) | 0,9998 | 0,4652 | 0,0012 | ** | ||
| 22 | Unconditional positive regard (Rogerian) | 0,9986 | 0,9998 | 0,0000 | *** | ||
| 24 | Biographical work (C, IBP, GES) | 0,6724 | 0,2774 | 0,0038 | ** | ||
| 27 | Interpretation ( PSA, SGBAT) | 0,9999 | 0,0163 | * | 0,0000 | *** | |
| 30 | Promoting insight into the necessity of behavior change (C, GES) | 0,9267 | 0,1936 | 0,0000 | *** | ||
| 31 | Empathy (C, Rogerian) | 0,8266 | 0,0801 | 0,0000 | *** | ||
| 32 | Working with boundaries, gradients of distance (IBP) | 0,0277 | * | 0,3176 | 0,0000 | *** | |
| 40 | Countertransference (C.G. Jung, PSA, SGBAT) | 0,9978 | 0,9999 | 0,0000 | *** | ||
| 42 | Purposeful frustration (SVG) | 0,3587 | 0,8835 | 0,1225 | |||
| 46 | Providing support (C, TA) | 1,0000 | 0,0000 | *** | 0,0000 | *** | |
| 52 | Providing information / giving advice (C, IBP) | 0,6859 | 0,0090 | ** | 0,0000 | *** | |
| 55 | Clarifying inquiry / exploration (C, GES, PSA) | 0,4627 | 0,0007 | *** | 0,0000 | *** | |
| 60 | Confrontation (PSA) | 0,9998 | 0,3444 | 0,0000 | *** | ||
| 65 | Working with metaphor (systemic) | 1,0000 | 1,0000 | 0,0833 | |||
| 69 | Positive reinforcement (CBT | 0,9996 | 0,1527 | 0,0000 | *** | ||
| 72 | Reframing (systemic) | 0,9229 | 0,0239 | * | 0,0001 | *** | |
| 75 | Resource activation (C, GES) | 1,0000 | 0,4486 | 0,0109 | * | ||
| 78 | Self-disclosure by the therapist (C ) | 0,3146 | 0,0668 | 0,0000 | *** | ||
| 80 | Creating meaning (SGAP, ISAP, C. G Jung Institute) | 0,9989 | 0,9027 | 0,0017 | ** | ||
| 85 | Addressing symptoms (C) | 1,0000 | 0,7267 | 0,0000 | *** | ||
| 87 | Changing the topic (C) | 0,9999 | 1,0000 | 0,0323 | * | ||
| 88 | Referring to the therapy contract (C, TA) | 1,0000 | 0,9999 | 0,0000 | *** | ||
| 89 | Addressing therapy goals (C, TA) | 1,0000 | 0,0001 | *** | 0,0075 | ** | |
| * = p < 0.05; ** = p < 0.01; *** = p < 0.001 | |||||||
| Art and Expression Oriented Therapy (EGIS), Bioenergetic Analysis (SGBAT), Cognitive Behavior Therapy (CBT), Existential Analysis and Logotherapy (GES), Gestalt Therapy (SVG), Integrative Body Psychotherapy (IBP), Process Oriented Psychotherapy (IPA), Psychoanalysis/Analytical Psychology (PSZ, SGAP, ISAP, C. G. Jung Institute), Transactional Analysis (SGTA/ASAT) | |||||||
Table 6. Comparison of Four Poisson Regression Models
4 multilevel regression models (see Bryk and Raudenbush, 1992) were computed, excluding intervention categories that were used in less than 10% of all sessions. One model included 3 (approach, therapist, patient), the other 3 models 2 random effects each (therapist, patient), (approach, patient), (approach therapist). The latter were compared with the first model including 3 factors, using the likelihood ratio test. Except for one single intervention category the use of interventions varied independently of therapists’ affiliation to certain types of psychotherapy. The factor therapist predicted the variability of intervention frequencies for 7 intervention categories. The factor patient was most informative for predicting the variability of intervention type frequencies. Table 6 presents the pertaining error probabilities.
3.3. Temporal Aspects: Descriptive
The same 10 intervention categories as the 10 most frequently used (69%) also filled 71% of the total session time investigated (see table 5, left and middle columns). At the same time we observed that intervals between interventions (the duration of intervention units) varied considerably within and across sessions.
In figure 2 the onsets of interventions in three different sessions are represented by horizontal bars along the continuum of time (y-axis).
Medians of interval durations for each type of intervention were computed. Categories having been employed less than 50 times in all sessions under study were excluded.
In a one-way analysis of variance types of intervention were not predictive for interval duration. But intervention categories could be arranged according to average interval duration following their use in descending order.
Especially specific intervention categories involved interactional units of longest durations. We created a time interval x intervention contingency table and computed chi-square values to determine which interventions led to lengthy interactions more frequently than would be expected by chance. Results identified the 10 interventions most likely to set off interaction units lasting longer than 120 seconds (see table 5, right column).
4. Discussion
Common intervention techniques are employed twice as often as compared to intervention categories specific to certain types of psychotherapy, roughly one and a half as many from other as from therapists’ own type of psychotherapy, which replicates findings by Lambert (1992). Eclecticism was clearly present. Therapists’ affiliation with different types of psychotherapy did not predict their interventional behaviour. Therapists seem to have developed personal styles which make their use of some types of intervention more likely than others. The factor patient however best predicted which types of intervention were employed, thus complying with Lambert’s (2013) and Norcross and Wampold’s (2011) request that therapists should try to match “techniques to client dispositions, personality traits and other diagnostic differences.”
Proponents of some approaches claimed interventions as specific to their type of psychotherapy, whereas in fact these were shared by all types investigated in our study (e. g., Psychoanalysis and Logotherapy claimed clarifying inquiry, Transactional Analysis claimed support, and Integrative Body Psychotherapy claimed providing information/giving advice as interventions specific to their approach. These four approaches have higher scores of “specific” interventions than the rest. In this light, differences in specificity between approaches seem to be largely due to different conceptualizations of specificity in different types of psychotherapy.
What cannot be observed are the concepts and strategies that therapists have in mind while they are interacting with their patients. Possibly these are relevant all the same. And from an external perspective, therapists’ concept orientation may have been underestimated. Common interventions may have prepared the ground for the attainment of type of psychotherapy-specific goals.
In almost all sessions there were sections in which the pace of patient-therapist interactions slowed down. Interventions that were followed by exceptionally long intervals to the next intervention were frequently specific interventions.
Interventions that mostly tended to slow down the pace of therapists’ interventional behavior were interventions specific to certain types of psychotherapy. Although their prevalence was not high, we think that these are worth investigating more closely. We suspect that prolonged interactional units could be indicative of change coming about in patients’ habitual patterns. Processing emotional irritation (Achtziger et al., 2014) or tasks of higher complexity take more time, as e. g. Sternberg (1975), Kintsch (1982), or Roth (1994) have pointed out. Verbatim transcripts done from our material also point into this direction.
The prevalence of 34% of specific interventions from different approaches, although eclectically applied, does not advise discarding the variety of different types of psychotherapy existing at present. On the contrary, the existing wealth of concepts and techniques should be acknowledged, carefully investigated, and integrated in therapeutic practice. It would probably be wise to acknowledge the role of common factors in effective treatments while also considering the usefulness of specific interventions from approaches that are not yet established as evidence-based.
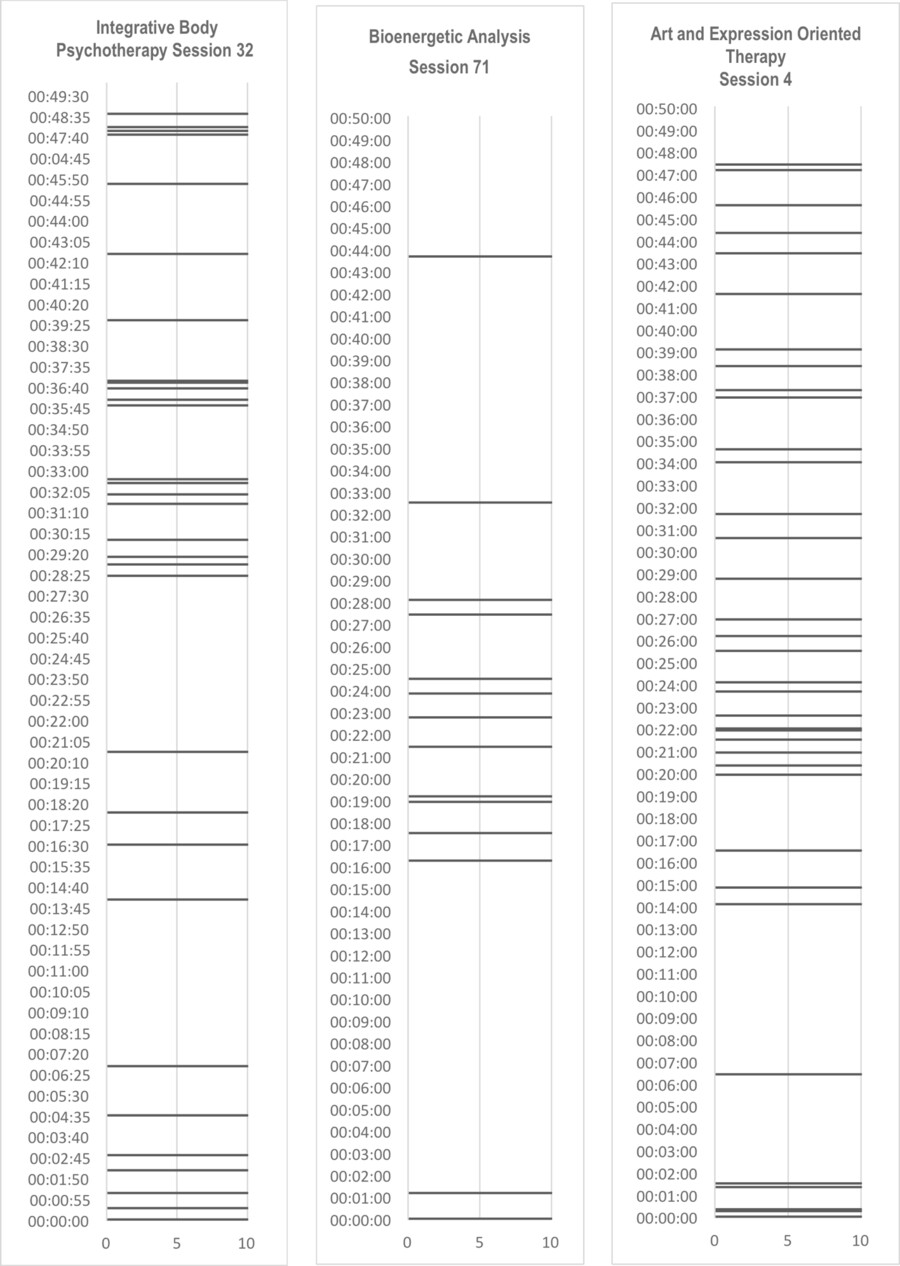
Figure 2. Varying pace of therapists’ interventional behavior in different sessions
Footnote
- [1]
- Brief Paper Presentation at the 8th European Conference on Psychotherapy Research, September 24th–26th, Klagenfurt, Austria.
References
Achtziger, A., Gollwitzer, P. M., Bergius, R. & Schmalt, H.-D. (2014). Motiv. In Wirtz, M. A. (Eds.), Dorsch. Lexikon der Psychologie. 17. Auflage (pp. 1113–1116). Bern: Huber.
American Psychiatric Association. (1989). Global Assessment of Functioning Scale. Diagnostische Kriterien und Differentialdiagnosen des diagnostischen und statistischen Manuals psychischer Störungen DSM-III-R. Weinheim: Beltz.
American Psychiatric Association. (1994) Diagnostic and Statistical Manual of Mental Disorders DSM-IV. Washington D. C.
Badalamenti, A. F. & Langs, R. J. (1991). An empirical investigation of human dyadic systems in the time and frequency domains. Journal of Behavioral Science, 36(2), pp. 100–114. https://doi.org/10.1002/bs.3830360204
Berne, E. (1961). Transactional Analysis in psychotherapy: A systematic individual and social psychiatry. New York, NY: Grove Press.
Bryk, A. & Raudenbush, S. W. (1992). Hierarchical linear models: Applications and data analysis methods. Thousand Oaks, CA: Sage.
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Hillsdale, NJ: Lawrence Erlbaum.
Crameri, A., von Wyl, A., Koemeda-Lutz, M., Tschuschke, V., & Schulthess, P. (2015). Sensitivity analysis in multiple imputation in effectiveness studies of psychotherapy. Frontiers in Psychology; https://doi.org/10.3389/fpsyg.2015.01042
Duncan, S. (1972). Some signals and rules for taking speaking turns in conversations. Journal of Personality and Social Psychology, 23(2), pp. 283–292. https://doi.org/10.1037/h0033031
First, M. B., Spitzer, R. L., Giblon, M. & Williams, J. B. W. (2012). Structured Clinical Interview for DSM-IV (SCID I and II). books.google.com (In German: Wittchen, H. U., Zaudig, M. & Fydrich, T. (1997). Strukturiertes Klinisches Interview für DSM-IV. Göttingen, Germany: Hogrefe. And: Saß, H., Wittchen, H. U., & Zaudig, M. (2003). Diagnostisches und Statistisches Manual Psychischer Störungen (DSM-IV-TR) [Diagnostic and statistical manual of mental disorders (DSM-IV-TR)]. Göttingen, Germany: Hogrefe.
Frankl, V. E. (1956–1999). Theorie und Therapie der Neurosen: Einführung in die Logotherapie und Existenzanalyse [Theory and therapy of neuroses: Introduction to logotherapy and existential analysis]. Munich: Ernst Reinhardt.
Freud, S. (1895–1940). Gesammelte Werke [Collected Works]: Vols. 1–17. Frankfurt: S. Fischer.
Hautzinger, M., Keller, F. & Kühne, C. (2006). BDI-II: Beck Depressionsinventar. Frankfurt, Germany: Harcourt Test Services.
Jung, C. G. (2000). Gesammelte Werke [Collected Works]: Vols. 1–20. Ostfildern, Germany: Patmos.
Kintsch, W. (1982). Gedächtnis und Kognition [Memory and cognition]. Berlin, Germany: Springer.
Knill, P. J., Nienhaus Barba, H. & Fuchs, M. (1995). Minstrels of Soul: Intermodal expressive therapy. Toronto, Canada: EGS-Press.
Koemeda-Lutz, M., Crameri, A., Tschuschke, V., Schulthess, P., & von Wyl, A. (2016 a, in print) Therapists’ interventions in different psychotherapy approaches Category and temporal aspects. International Body Psychotherapy Journal
Koemeda-Lutz, M., Crameri, A., Schulthess, P., von Wyl, A., & Tschuschke, V. (in print) Specificity and Pace Variability of Therapists’ Interventions under Naturalistic Conditions. International Journal for Psychotherapy
Lambert, M. J. (1992). Psychotherapy outcome research: Implications for integrative and eclectic therapists. In J. C. Norcross & M. R. Goldfried (Eds.), Handbook of psychotherapy integration (pp. 94–129). New York, NY: Basic Books.
Lambert, M. J. (Eds.). (2013). The efficacy and effectiveness of psychotherapy. In M. J. Lambert (Ed.), Bergin and Garfield’s Handbook of Psychotherapy and Behavior Change (6th ed.), (pp. 169–218). Hoboken, NJ: John Wiley & Sons.
Landis, J. R. & Koch, G. G. (1977). The measurement of observer agreement for categorical data. Biometrics, 33(1), pp. 159–174. doi:10.2307/2529310
Langs, R. J. & Badalamenti, A. F. (1990). Stochastic analysis of the duration of the speaker role in psychotherapy. Perceptual Motor Skills, 70, pp. 675–689. https://doi.org/10.2466/pms.1990.70.2.675
Lowen, A. (1958). The Language of the Body. New York: Prentice Hall.
Mindell, A. (1998). Dreambody. Portland, OR: Lao Tse Press.
Norcross, J. C., & Wampold, B. E. (2011). What works for whom: Tailoring psychotherapy to the person. Journal of Clinical Psychology: In Session, 67(2), 127–132. https://doi.org/10.1002/jclp.20764
OPD Task Force. (Ed.) (2001). OPD Operationalized Psychodynamic Diagnostics: Foundations and practical handbook. Bern, Switzerland: Hogrefe & Huber. (In German: Arbeitskreis OPD. (Ed.). (2006). Operationalisierte Psychodynamische Diagnostik OPD 2: Das Manual für Diagnostik und Therapieplanung. Bern, Switzerland: Huber)
Perepletchikova, F., Treat, T. A. & Kazdin, A. E. (2007). Treatment integrity in psychotherapy research: Analysis of the studies and examination of the associated factors. Journal of Consulting and Clinical Psychology, 75, pp. 829–841. doi:10.1037/0022-006X.75.6.829
Perls, F. S., Hefferline, R. F. & Goodman, P. (1951). Gestalt Therapy: Excitement and growth in the human personality. New York: Julian Press.
Rochet-Capellan, A. & Fuchs, S. (2014). Take a breath and take the turn: How breathing meets turns in spontaneous dialogue. Retrieved from rstb.royalsocietypublishing.org
Rosenberg, J. L., Rand, M. L. & Asay, D. (1996). Körper, Selbst und Seele: Ein Weg zur Integration [Body, self, and mind: A way to integration]. Paderborn, Germany: Junfermann.
Roth, G. (1994). Das Gehirn und seine Wirklichkeit: Kognitive Neurobiologie und ihre philosophischen Konsequenzen [The brain and its reality: Cognitive neurobiology and its philosophical consequences]. Frankfurt, Germany: Suhrkamp.
Sternberg, S. (1975). Memory scanning: New findings and current controversies. Quarterly Journal of Experimental Psychology 27, 1–32. https://doi.org/10.1080/14640747508400459
Tschuschke, V., Crameri, A., Koehler, M., Berglar, J., Muth, K., Staczan, P., von Wyl, A., Schulthess, P. & Koemeda-Lutz, M. (2015) The role of therapists’ treatment adherence, professional experience, therapeutic alliance, and clients’ severity of psychological problems Prediction of treatment outcome in eight different psychotherapy approaches. Preliminary results of a naturalistic study. Psychotherapy Research, (25) 4, 2015, 420–434
Tschuschke, V., Koemeda-Lutz, M., & Schlegel, M. (2014). Ratingmanual für psychotherapeutische Konzepttreue: Praxisstudie ambulante Psychotherapie Schweiz (PAP-S) der Institute der Schweizer Charta für Psychotherapie [Rating manual for psychotherapeutic treatment adherence: Practice Outpatient Psychotherapy Study Switzerland (PAP-S) of the Institute of the Swiss Charta of Psychotherapy].
von Wyl, A., Crameri, A., Koemeda-Lutz, M., Tschuschke, V., & Schulthess, P. (2013). Praxisstudie ambulante Psychotherapie Schweiz (PAP-S): Studiendesign und Machbarkeit [Practice Outpatient Psychotherapy Study Switzerland (PAPS): Study design and feasibility]. Psychotherapie-Wissenschaft, 1, 6–22.
About the Authors
Margit Koemeda-Lutz: PhD, psychologist, psychotherapist and faculty member of the IIBA; coordinating trainer for the SGBAT (Swiss Society for Bioenergetic Analysis and Therapy). Co-founding member of the PAP-S research group.
E-mail: koemeda@bluewin.ch
Aureliano Crameri, MSc, is a PhD candidate, research associate, psychologist, quality manager, and academic instructor of research methodology at Zurich University for Applied Sciences.
E-mail: aureliano.crameri@zhaw.ch
Peter Schulthess, MSc, is an instructional therapist and psychotherapist; education leader at the Institute for Integrative Gestalt Therapy Switzerland; and president of the Swiss Charta for Psychotherapy
E-mail: praesidium@psychotherapiecharta.ch
Agnes von Wyl, PhD, is a professor, psychologist; lecturer; and head of the Research Unit for Psychotherapy and Mental Health at Zurich University for Applied Sciences.
E-mail: vonw@zhaw.ch
Volker Tschuschke, PhD, is a professor, professor emeritus, psychologist, psychoanalyst, formerly head of the department of Medical Psychology at the University Hospital of Cologne, Germany; currently head of the graduate program in psychology at the Sigmund Freud Private University, Berlin.